Trumpism is a toxic brew of hyper-tribalism, hyper-individualism, and dogmatic false certainty. Let’s first distinguish between “Trumpism” and “Conservatism.” There is some overlap, and there are some conservative (as well as, frankly, some liberal) ideas in the mix of Trumpism that are simply bad ideas in their own right, but Trumpism distinguishes itself by being almost entirely toxic, with very few glimmers of well-conceived and generally beneficial aspects to it. Conservatism covers a wide range, including many of the elements that go into Trumpism, but it isn’t inherently or inevitably anti-intellectual; it isn’t inherently or inevitably anti-fact or anti-reason; it isn’t inherently or inevitably religiously fanatical; it isn’t inherently or inevitably anti-Latino or anti-Muslim or anti-Black; and whatever of Conservatism is left after filtering those toxic elements of Trumpism out is the governing partner this country needs and deserves and this world requires of us.
We can examine this toxic mix of hyper-tribalism and hyper-individualism in relation to virtually any issue we face, but one that gets at its essence and is repeatedly, tragically, brought to the fore is the debate over gun violence in America, and particularly mass shootings. Guns aren’t the underlyng problem (though they are the most immediately tractable causal link). The combination of hyper-individualism and hyper-tribalism is the underlying problem (as it generally is).
At the time of this writing, we are in the wake of yet another mass shooting (two, in fact, occurring with 24 hours of each other). One of these recent shootings was carried out by a Trump supporter echoing Trump’s language and targeting a group Trump has consistently and relentlessly vilified. Every Trumpist insisting that the shooting in El Paso was in no way Trump’s fault insists that it is ONLY the shooter’s fault, or the shooter’s fault and the fault of society at large for failing to deal with mental health issues more effectively. By that logic, ISIS inspired lone-wolf terrorism isn’t ISIS’s fault; it’s either only the lone-wolf terrorist’s fault or the fault of OUR society (when the ISIS inspired terrorist is residing here) for failing to deal with mental health issues more effectively. Let’s examine both of those claims, determining how evenly they are applied, with how much integrity they inform ideological positions as a result of being applied, and the systemic ways in which they are or are not applied depending on other variables.
The illogic of hyper-individualism isn’t applied evenly; it’s applied conveniently. When something happens because of systemic or non-proximate causes that Trumpists, for ideological reasons, do not want to address, it is the individual –the proximate cause– who (according to Trumpists) bears all of the responsibility, but when something happens because of (real or imagined) systemic or non-proximate causes that Trumpists want to address, entire races are to blame. In other words, they are hyper-individualistic in terms of shouldering responsibility for what members of their own tribe do at the instigation of their own tribal leader (“it’s not our responsibility or Trump’s responsibility; it’s just the shooters responsibility”), but hyper-tribalistic when allocating responsibility for what members of other tribes do (“Muslims are out to get us! Mexicans are rapists and murderers!”).
Hyper-tribalism attributes every bad act by any out-group member to all of the out-groups in their entirety to which that individual belongs, while selective hyper-individualism allows the absolute hypocrisy of attributing any bad act by any in-group member to that individual alone while insisting that the rest of the in-group is blameless even if there is direct evidence of blame elsewhere within that group (such as Trump’s and Fox News’s incitements).
When Tumpists insist that the real problem is a mental health problem –despite that not generally being the case in the clinical sense of the term “mental health”– they are protecting their tribe by invoking some non-tribal force at play instead, but, even if that non-tribal force were really the pivotal causal factor, the selective hyper-individualism of their tribe kicks in and perpetually obstructs efforts to address things like mental health in a publicly funded way, because that is “too much government.” And, in fact, there are indeed societal factors in play, things we as a society could address if we were willing to be more proactive and less reactive, more aware of our interdependence and less hyper-individualistic, but which the same faction that refuses to allow us to address the role that guns play refuses to allow us to address as well.
The hyper-individualism also allows gun idolaters to focus exclusively on the individual pulling the trigger, and not on the role that our gun laws play in giving him a trigger to pull. The role that guns play as the fetish of this tribe, the totem at whose altar they worship, increases the incentive to mobilize the hyper-individualism in service to this farce, such that it is impossible to penetrate the demonstrably false narrative with fact and reason.
This combination of hyper-individualism and hyper-tribalism on the Trumpist right has become the perfect toxic storm, one which is already doing serious harm to large numbers of people and is placing our national and world in serious danger. True patriots find the courage and integrity to reassess and redirect themselves, for the good of their fellow countrymen and their fellow human beings. It’s time for Trump supporters to become true patriots and, frankly, stop supporting this toxic walking disaster of a president. Conservatism deserves a better leader.
All decent human beings, all people who care about both the economic health of this country and the values it stands for, should reject, resoundingly, the nativist xenophobia hawked, cynically, by the current president to a tragically receptive segment of our population. Illegal immigration is less than one fifth of what it was 20 years ago, and reached that low mark prior to Trump’s election. Our border security is quite sufficient, in reality, with crime rates by illegal immigrants being lower than crime rates by natural born citizens and crime rates by geographic locale being inversely correlated to the proportion of the population that are immigrants in that locale (i.e., more immigrants = less crime). Those are statistical facts.
There is absolutely no evidence that even a single terrorist has ever come across our southern border, according to Trump’s own justice department. The 4000 number that Sarah Huckabee Sanders used refers to people arriving at airports from countries that we consider to be countries that terrorists frequently hail from; they are not even suspected of terrorism, and they do not come across the southern border. In fact, the justice department and anti-terrorism experts in general consider the Canadian border to pose a greater danger of providing a conduit for terrorists, because there is much more radical Islamic influence in Canada than in the Latino countries south of us.
It’s also a fact that at a certain point further investment in border security costs more per person successfully prevented from crossing the border illegally than that person costs us if they do cross the border illegally. In fact, it’s extremely likely that we have already passed that point. Non-partisan analyses of the costs and benefits that illegal immigrants provide to our coffers and our economy range from net benefits on both scores at both the state and federal levels to fairly marginal net costs on both scores. No peer-review study has come to the conclusion that costs are any significant portion of GDP, or that they are anywhere near posing an economic crisis to the country.
Conversely, that which is currently illegal immigration DOES redress a critical and rapidly growing demographic imbalance between retirees drawing out of pension funds and working people paying into them. Developed countries really have little choice, if they want their pension funds to remain solvent, but to legalize and normalize fairly massive immigration of working age people.
Furthermore, the argument that the nativism and xenophobia on very prominent and obvious display by this president and his followers is just a commitment to the rule of law, not an anti-immigrant stance, is belied by both the nature of the issue and the facts. We determine what the laws are, and virtually everyone agrees that we need immigration reform, which means changes in the laws. So the real debate is over what the laws should be and how we should implement them. The divide in the debate is between those who favor a kinder and more open society and those who favor a crueler and more closed society.
That it isn’t just, or even primarily, about enforcing current laws is highlighted by the fact that when Trump proposed changes in the law to make immigration more restrictive and favor “Norwegians” over people of color, and when crueler and more restrictive choices of policy not dictated by currents law were implemented, his supporters passionately supported and defended his choices, demonstrating that the debate isn’t over enforcing the law but rather shutting out precisely the people we used to welcome.
Those who echo Trump’s narrative on immigration often compare the nation to a house, insisting that just as we use walls and locks to exclude people at will from our homes we should do so to exclude them from our country. It is redundant at this point to address the ineffectiveness of a wall (something a review of expert analyses of border security makes perfectly clear), so instead let’s focus on the errors in that analogy.
A country isn’t a house. It wasn’t legally purchased from its previous owners; it was stolen. Its property lines aren’t determined by developers selling lots; they’re determined by military conquest. Its walls don’t separate inhabitants from the elements, but rather secure those who managed to divert more of the Earth’s resources to themselves against those who have been violently relegated to diverting less to themselves. And it is not a refuge from the world financed by inhabitants’ labors external to it, but rather a complex economic, social, and cultural entity that thrives by means of its robust interactions with the world around it.
Let’s address the last point first, because it is the one that cuts across values and appeals directly to systemic realities. Our nation functions through an internal and external market economy, engaging in market exchanges within our borders and across borders. Classical (and conservative) economic theory maintains that the fewer barriers there are to such market exchanges, the more wealth is generated by them, the ideal being a “free market,” characterized by unhindered market activity. Advocacy for strengthening national borders and obstructing the flow of people across them is a contradiction of this ideal. Less ideologically pure understandings of market dynamics also recognize the value of allowing labor to travel to where there is demand for it. Whatever limits we feel we must place on that free flow of goods and people in service to a free market, the fact that it is a consideration is one of the principal ways in which a country differs from a house, not just on scale, but also in systemic attributes.
But a country differs from a house in other ways as well, on moral and historical dimensions. We can’t return land to all those with historical claims on it, but we can stop pretending that we have some absolute, inherent moral authority to deprive entry to those who are the descendants of the ones we stole it from seeking to work hard and provide opportunity for their children under our rule of law. Those who *have* always pass laws to protect what they have from those who don’t; one can defend that through a cynical insistence that might makes right but not through a claim to having the morally virtuous position. The morally virtuous position would be to recognize our moral debt to humanity as a result of the historical moral infractions through which we secured our privileged place in the global political economy.
And it’s a pretty easy form of “generosity” to let hard working people come here and do our dirtiest, most difficult jobs for the lowest wages, contributing to our economy, to our coffers, and to our culture. The fact is that most analyses show net gains to our economy, many show net gains to our state and federal coffers, and all show a net gain in our demographic distribution of workers to retirees, a critical imbalance at present that massive immigration redresses.
You people who think we should wall out the less fortunate because you feel threatened by them are the least fortunate of all, coveting material wealth that isn’t being threatened by inflicting passive and active brutalities on those most in need. You’re not Christians; you’re what Christians exhort us not to be.
This entire nativist, xenophobic narrative is a fabrication, refuted by fact, by reason, by our own national interests, and by basic human decency. And it is one that an opportunistic con-artist has leveraged, as he’s leveraged other similarly dishonest scams before, to stoke up the bigotries of a certain segment of our national population in order to serve his own personal self-aggrandizement.

An alternative representation, to emphasize the “flor”
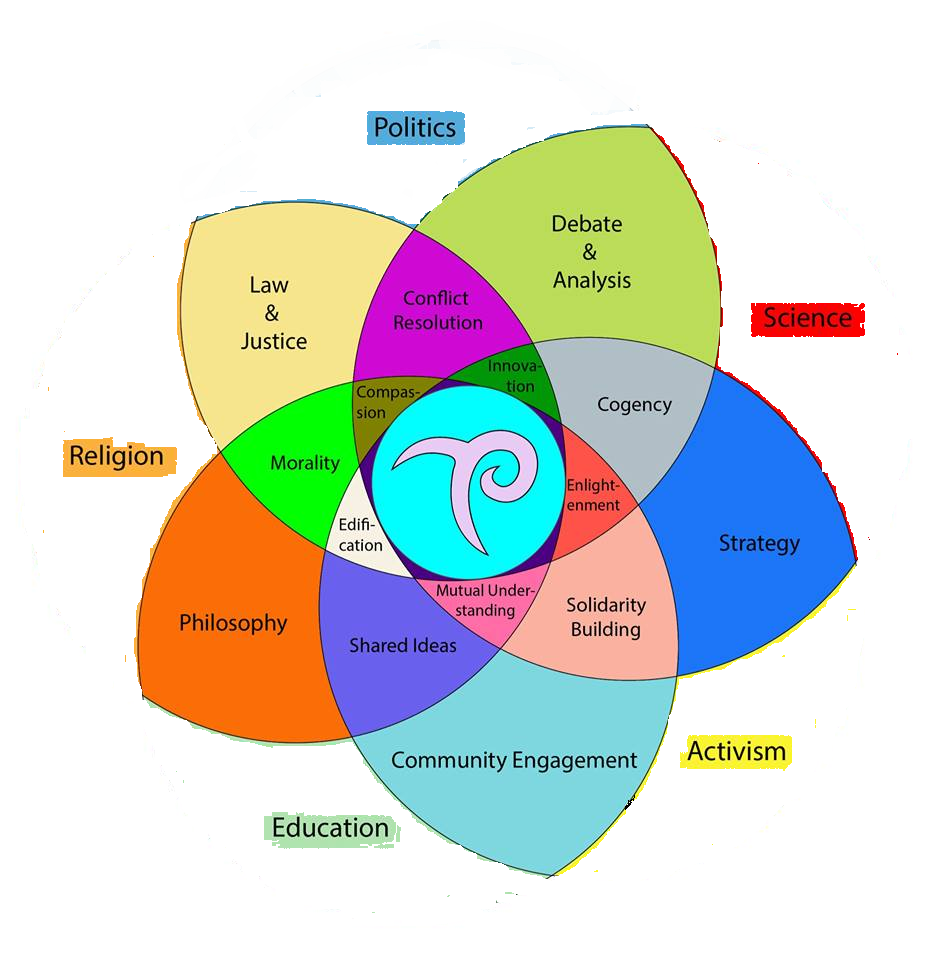
The Flor de Luz, the Flower of Light, is both a symbol and, potentially, a tool. It is the symbol of Transcendental Politics (and logo of The Transcendental Politics Foundation) found in the middle of this Venn diagram, and the diagram itself. The name is, in part, a play on words of the French “Fleur de Lis” (a stylized lily), recognizing the incidental similarity of the original logo to a luminescent lily. It is also in part a reference to the concentric flower patterns formed by the overlapping circles of the Venn Diagram, with five small petals surrounding the logo, five larger ones surrounding those. and five larger ones still surrounding those (see the alternative representation). Most importantly, it is a reference to what both the logo and the Venn Diagram represent: Transcendental Politics, the flowering (“flor”) of a new Enlightenment (“luz”).
The Flor de Luz is, in one sense, a simple graphic with a simple purpose. It represents how Transcendental Politics resides at the confluence of our various overarching social institutions, how it aspires to be a distillation and synthesis of what is best in each of them, what has thus far worked well for humanity, leaving out what is least useful in each of them, what has thus far not served humanity well, an ongoing social movement that recognizes and respects the cumulative product of human history and humbly but proactively builds on it, weeding and pruning and watering portions of our social institutional landscape with new layers of conscious cultivation, continuing the human enterprise of transforming the wilderness of what time and numbers have produced into a garden of intentionality that better serves human welfare.
But the Flor de Luz is, in another sense, potentially (in a dynamical form discussed below) something more subtle and complex, a conceptual tool to assist in the identification stage of that ongoing endeavor of social institutional distillation and synthesis, a tool that is only partially and statically represented by the Venn Diagram above. Let’s explore, step-by-step, how it might be transformed into a dynamical tool.
First, consider possible variations of the Venn Diagram above. A different arrangement, or sequence, of the same five circles could be chosen, different pairs overlapping in the outermost petals (e.g., placing politics and activism next to each other, and religion and science next to each other, producing in their overlaps “campaigning” and “pursuit of universal paradigms,” respectively); or different overarching institutions altogether could be chosen (e.g., economics, family, technology, energy, environment, fine arts, etc.), creating a proliferation of possible combinations and sequences. (For instance, one product of the overlap of activism and economics might be “entrepreneurialism,” and of entrepreneurialism and technology “innovation,” leading to one of the already identified smaller petals by a different route.) Different aspects of what their convergences create can be highlighted, illustrating, in a sense, how “all roads lead to Transcendental Politics,” to the commitment to foster a more rational, imaginative, empathetic, humble and humane world.
We can create a completely different kind of Flor de Luz comprised of cognitive and emotional modalities instead of social institutions, with, for instance, reason, imagination, empathy, humility, and humanity (the five core values of Transcendental Politics) as the five overlapping circles, producing social institutions and types of behaviors and endeavors. We can even include such emotions and modalities as anger, fear, and tribalism, things we usually identify as that which we are striving to transcend, to acknowledge that they too have evolved for reasons, and that they may well have something to contribute to our garden of intentionality. Or we can combine cognitive and emotional modalities with social institutions from the outset, testing our minds to identify, for instance, what good can be harvested from the distillation and synthesis of anger, reason, and activism, or of imagination, fear, hope, and science, or of the convergence of those two sets. The possibilities are nearly limitless.
The purpose of presenting ourselves with these nearly limitless combinations is to guide our minds in an exploration of what is, in pursuit of what can be, by facilitating consideration of how we can work to leverage what is into something more beneficial. This can occur both in the abstract, imagining possibilities without worrying about how to attain them, and in the particular, identifying viable pathways to implementation and devising first steps that can be taken now in service to that end. It is, if nothing else, a tool for taking our minds out of the tumultuous onslaught of the perpetual urgency of now, and providing them with a space defined by a more synoptic view, in which we are guided not only in “thinking outside the box,” but in redefining “the box” as something far more expansive.
(I should insert here a response to the criticism, that I imagine has arisen in the minds of at least some readers by now, of “what does this have to do with anything? How does combining names of social institutions and cognitive and emotional modalities accomplish anything?” The answer is that it displaces our tendency to think in fixed ways determined by ideological narratives and ingrained habits of thought with a set of semi-random but also subtly systemic prompts to think in new ways. That can be remarkably useful, and it is integral to the meaning of “Transcendental Politics,” which is about institutionalizing the ongoing effort to transcend our ideological tribalisms and false certainties.)
Let me guide you through a consideration of how this design (five overlapping disks representing distinct social institutional, cognitive, and emotional modalities) can be utilized in the manner described above.
Imagine a narrated animation in which, first, the diagram is explained as representative of how Transcendental Politics is that which resides where our social institutional modalities overlap, each mitigating the others’ defects and reinforcing the others’ strengths, a sort of distillation of the best of what we’ve produced over the millennia, the product of the spinning lathe of trial and error. Then, the outer sections labeled “science, politics, education, activism, religion” are removed and the largest flower pattern is revealed, the narration stating that even though the various institutional modalities themselves are not precisely what Transcendental Politics is (because they exist independently), those aspects of their synthesis that are relevant to serving our shared humanity most effectively are distilled into the Flor de Luz. Then the next layer of petals is removed, and the next, and the narration continues, focusing on the distillation down to those essential ingredients that define Transcendental Politics, bringing the narration to a focus on precisely what Transcendental Politics IS, that quintessence at the center of this convergence of social and cultural evolution.
The animation can then grow back outward, with new petals labeled with new virtues distilled from other arrangements, both in sequence and in selection, of overarching institutions and modalities until a new completed Flor de Luz is constructed, the narration describing along the way how the petals of the concentric flowers, which in the other direction were derived from the larger overlapping petals, in this direction are emergent from the smaller ones (and ultimately from the center, from Transcendental Politics), illustrating how it inherits the cultural material of the past and helps create the cultural material of the future. The animation can then proceed to to a sliding around of the overarching circles, with the petals formed by their new overlaps changing accordingly, and then to a changing of the overarching institutions and modalities themselves, exploring some of the many different permutations of the Flor de Luz.
Now imagine a physical artifact, with five overlapping translucent plastic or glass colored circles in the form of the Flor de Luz, each rotatable around its center and able to switch positions by pivoting around the center circle containing the TPF logo and snapping into a new position. Each disk would contain perhaps three related social institutions or cognitive or emotional modalities that can be rotated into place, creating the possibility for 15 different arrangements without moving the relative positions of the disks, and some multiple of that by moving the relative positions of the disks. A complete set of disks can include far more than five, with the ability to switch out individual disks for others, removing all limits on how many arrangements can be explored. Of course doing so only suggests the combinations; the work of thinking about what that implies, what productive uses those combinations have, remains. But that work, too, can be cataloged and accumulated, in a kind of ongoing “social institutional genome project.”
(We can even create disks whose overarching categories are the finer ones produced by the confluence of other disks, and take their confluence into deeper, finer, and subtler levels.)
In an online version, that cumulative work can result in different combinations leading to different implied products of those combinations appearing in the various petals of the flower (much as they do in the graphic above). The physical artifact might accomplish the same through symbols visible in each petal in each rotational position of the disk, depending on which overarching principle is in effect, forming a sequence with the others, and then using a reference manual to interpret different sequences of symbols, the reference manual itself being a cumulative compendium of previous thought about the various possible combinations. Thus, this device could be used to explore different configurations of overlapping social institutional, cognitive, and emotional modalities, as a useful analytical and practical tool for thinking about how we can create different kinds of collaborative projects using those modalities in service to working our way toward the convergence in the center (Transcendental Politics).
(I can imagine turning it into a game as well, one that exercises the mind in certain ways that are aligned to what we are trying to cultivate, in which in each player’s turn they are challenged to take the set of social institutions and cognitive modalities they get from their “spin” of a Flor de Luz designed for that purpose and either create something from it following a set of rules and in pursuit of a defined goal, or build on what previous players have created. This is, obviously, not a fully fleshed out idea yet; just a glimpse of another possible use.)
What the Flor de Luz thus represents is that we have inherited an enormous quantity of social institutional, technological, cultural, cognitive, and emotional material, that is blended and can continue to be blended in complex ways, and that forms an evolving shared cognitive landscape of enormous complexity, subtlety, and power. It represents that we are not merely passive recipients of this material, but rather active participants in its ongoing formation, in how we combine and distill it, in what we derive from it, in how we employ it, in short, in what kind of world we choose to create together.
The Flor de Luz provides us with a relatively simple but elegant tool for thinking about this, for focusing our thoughts in productive ways. It reminds us of the possibilities, of how religious material and scientific material can combine beneficially, of the need to draw on reason and imagination and empathy all at once and not to pretend that anger and tribalism can (or should) just be wished away, of where our shared stories come from and what purposes they can serve. It reminds us of the fractal geometry of the anthrosphere, of how social institutional and cognitive and emotional materials are tributaries to larger streams; it helps us to reconstruct those tributaries and streams and rivers of possibilities in endless combinations. It is not a necessary tool; we can engage in the same contemplations without it. But it assists us in doing so more comprehensively and more precisely. Think of it as a social institutional kaleidoscope, with mechanisms for considering every set of combinations of every set of cognitive, emotional, and social institutional materials, and thinking about what those combinations imply, what challenges and possibilities they pose, what opportunities they present.
While potentially useful, it is certainly not a sufficient tool in and of itself; in the forthcoming book, “Transcendental Politics: A New Enlightenment,” I go into considerable detail exploring some small portion of the corpus of analytical and practical tools that are relevant to our endeavor. The need to continue to gather, produce, and synthesize them is perpetual. But the Flor de Luz is a reminder that at the core of all of that intellectual material and practitioner expertise are the lessons of our ongoing history, the convergence of a history of past experiments, and the cumulative products of human genius forming the foundation of present and future innovations. It is up to us to design those innovations to most effectively serve the ever fuller realization of our consciousness and of our shared humanity.
Our various personalities and affinities are reflected in which petals of which variations of the Flor de Luz resonate most with our own predispositions, talents, and desires; it becomes a way of locating ourselves in this shared endeavor of ours, of thinking about who our social institutional neighbors and natural partners are, of who we can reach out to to create new synergies in service to our shared humanity, to the greatest realization of our consciousness and our well-being, individually and collectively. It recognizes both diversity and coherence, facilitates both, draws upon both. The Flor de Luz is a way of thinking about our various roles in this shared story we are living and writing together, and how we can each individually and in cooperation with others, consciously and conscientiously, ensure that we are writing it and living it well.
To learn more about Transcendental Politics and The Transcendental Politics Foundation, visit our Facebook group, our Facebook page, or our website (still under construction).
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
Mischievous imps blowing invisible darts that stoke human passions and spin them out of control, moving twigs a few inches across the forest floor providing links in conflagrations that would not otherwise occur, plucking the strings of nature to produce crescendos of catastrophe. Zen-mathematician wizards dancing in their ice spheres high in the Vaznal Mountains, solving ever-deepening riddles of sound and sight and sensation, weaving order from the chaos the Loci imps foment. Winged muses carving sensuous stories from the clouds and celebrating the lives of those from whose dreams and tribulations they were born.
A fiery giantess is held captive in a hollow mountain. A sea serpent’s breath inspires the priestess of an island oracle poised above a chasm beneath which it sleeps. City-states are at war; slaves, led by a charismatic general, are in uprising; dictators and warlords are vying for power; neighboring kingdoms and empires are strategically courting local clients in pursuit of regional hegemony or outright conquest. Human avarice has strained the natural context on which it thrives. And ordinary people in extraordinary times, caught within the vortex of the powers that both surround and comprise them, navigate those turbulent currents.
Follow the adventures of Algonion Goodbow, the magical archer; Sarena of Ashra, the young girl at the center of this epic tale; their friends and mentors, guides and adversaries, as they thread the needle of great events, and discover truths even more profound than the myths of legend and lore. Discover the truth of fiction and the fiction of truth; celebrate the fantastic and sublime, in this magical tale laden with rich echoes of world history and world mythology, informed by blossoms of human consciousness from Chaos Theory to Thomas Kuhn’s theory of paradigm shifts, from Richard Dawkin’s Meme Theory to Eastern Mysticism, enriched by the author’s own travels and adventures.
A prophesied Disruption is upon the land of Calambria, causing the Earth to quake and societies to crumble. The Loci imps are its agents, but, according to Sadache mythology, it is Chaos, one of the two Parents of the Universe, who is its ultimate author. As Chaos eternally strives to make the One Many, Cosmos, the other Parent of the Universe, strives to make the Many One. The Sadache people view themselves as the children of Cosmos, whom they worship, and the lowest rung of a hierarchy of conscious beings opposing Chaos and the Loci imps. Above them, both of them and apart from them, are the drahmidi priests of the Cult of Cosmos, founded by the hero and conqueror Ogaro centuries before. Above the drahmidi are the Vaznallam wizards, Cosmos’s agents, just as the Loci are Chaos’s.
As the Great Disruption begins to manifest itself, Sarena of Ashra, a peasant girl from a village on the outskirts of the city-state of Boalus, flees an unwanted marriage to an arrogant lord and in search of freedom and destiny. She meets a young vagabond on the road, coming from the seat of the ceremonial High Kingdom, Ogaropol, fleeing his own pursuers. Together they form an alliance that leads through adventures together and apart, and binds them into two halves of a single whole.
Swirling around them are the wars of would be dictators and cult-leaders, of neighboring empires and kingdoms; the adventures of young Champions engaged in the prophesied Contest by which the Redeemer would be chosen and the Realignment realized. But, in both different and similar ways, the culmination of centuries of history flows through these two people, Algonion and Sarena, on haphazard quests of their own. And both the past and the future are forever changed by their discoveries and deeds.
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
Click here to learn about my mind-bending epic mythological novel A Conspiracy of Wizards!!!
The Child Welfare through Family and Community Facilitation Act (the Act):
(1): The Family and Community Facilitation and Child Welfare Administration (the Administration) shall be established to execute this Act and all of its provisions.
(a): The Administration shall be staffed by Community Facilitators (CFs) and Family Support Case Workers (FSCWs), trained and licensed in the skills necessary to implement the provisions of this Act.
(2): Current Parents, Expectant Parents, Foster Parents, Prospective Adoptive Parents, Legal Guardians, or primary care-givers (collectively, “parent,” whether referring to one parent acting alone or more than one parent making decisions together), along with their children, shall either formally belong to a Community, as defined in subsection (a), and participate in Community Parenting Support Meetings (CPSMs), or shall attend a Parental State-Disengagement Determination (PSDD) conducted by an agent of the Administration according to section 2(c) below. (Non-parents are encouraged, but not required, except as specified below, to belong to a Community and attend CPSMs). If a parent declines to attend either CPSMs or a PSDD, then an FSCW will automatically be assigned to that parent.
(a): The Administration shall create regulations to ensure that parents, both expectant and actual, follow procedures incumbent on parents in accord with this Act as soon after being informed of impending or actual parenthood, or beginning adoption proceedings, as is reasonably practicable.
(b): A Community, for the purposes of this statute, is either geographically or culturally defined.
(i): A parent shall by default belong to his/her geographical community, unless that parent selects a cultural community to belong to.
(ii): The upper and lower numerical limits of such Communities, the boundaries of Geographical Communities, the degree of geographic dispersion permissible for Cultural Communities, and the criteria of what constitutes a Cultural Community, shall be determined by the Administration according to guidelines designed to ensure that each Community is so constituted as to be capable of satisfying the functions described in the provisions of this Act, and of advancing the goals defined as the purpose of this Act (following the provisions described in subsection (iii) to protect parents utilizing culturally variant practices from ethnocentric presumptions of abuse or neglect).
(iii): Culturally variant practices that might be technical violations of the law, or presumptively harmful from a prevalent American cultural perspective, shall constitute grounds neither for refusing definition to a Cultural Community, nor for invoking the provisions in sections 4 and 5 of this statute, if they do not unambiguously create objective harm or deprivation to the child, if all or nearly all members of the Cultural Community would find the practice harmless and inoffensive, and if the Cultural Community has an independent existence and is not an artifact of convenience designed primarily to insulate its members from legal constraints to which they would otherwise be subject.
(iv): Communities shall be assigned the task of ensuring, with the organizational resources allocated and with the oversight of the CF, that the basic needs of parents and children in the Community are attended to by
(I): assisting parents in accessing the relevant family support programs established by complementary legislation, which provide children and families with adequate material support and vital services,
(II): facilitating mutual cooperation among Community members to provide one another with the moral, emotional, and informational support conducive to the long-term welfare of all of the children and parents in the Community, and
(III): providing children with age-appropriate means for expressing their views and preferences regarding their own upbringing and disposition, and having those views and preferences known and taken into consideration in any proceedings that involve them.
(c): CPSMs shall be held at a frequency to be determined by the Administration for each Community in consultation with the members of that Community, not to exceed one time per week nor be less than one time per month. By similar means, the Administration shall establish a mandatory attendance rate for parents in each Community, not to be less than 30% nor exceed 70% of all meetings, applicable to each parent individually, except in particular cases in accordance with subsection (ii) below.
(i): Each Community shall arrange on-premises child-care during the meetings by having three or more parents, on a rotating basis, undertake child care responsibilities during each meeting.
(ii): The Administration shall assist individual parents and Communities to make special arrangements in cases of particular scheduling problems, exercising a substantial commitment to accommodating parents with such verified scheduling problems, so long as the conflict involves an obligation that substantially contributes to the family’s material welfare.
(d): The Administration shall conduct PSDDs at the time and location most convenient for the parent whenever possible, and with substantial deference to the parent’s presumed right to direct the upbringing of the parent’s child(ren) as the parent sees fit. The Administration shall determine at the PSDD whether there is any compelling reason not to permit the parent to voluntarily disengage from the Family and Community Support apparatus established by this Act.
(i): The Administration shall establish a fully delineated set of criteria by which to make such determinations, and will do so under guidelines designed to prevent the influence of prejudices on the part of its agents, such as those regarding race, ethnicity, culture, class, gender, or sexual orientation.
(ii): If such a compelling reason is not found to exist, the parent will be allowed to disengage from the state involvement delineated in this Act, except for the provisions of sections 2(d), 3(a)(5), 5, and 6.
(iii): If such a compelling reason is found to exist, the parent will be assigned an FSCW.
(3): Family Support Case Workers (FSCWs) are entrusted with the responsibilities of monitoring families for evidence of Child Abuse or Neglect (as defined in 20-8-140 of the SHF Revised Statutes); working with parents (always deferential to parents’ preferences short of child abuse or neglect) and children to improve coping skills and devise more effective strategies to deal with the challenges of child-rearing; identifying particular family problems, challenges, and needs that are having or can reasonably be expected to have a significant impact on the child’s welfare; and recommending to the Administration interventions and assistance that are conducive to the continued provision of a safe and healthy home environment for the child.
(a): An FSCW shall be assigned to a parent when
(i): a parent requests it,
(ii): a Community Facilitator (CF) recommends it,
(iii): the Administration deems it necessary through a Parental State-Disengagement Determination,
(iv): a parent declines to participate in CPSMs or, alternatively, to attend a PSDD,
(v): the Administration deems it necessary as the result of an investigation into an allegation of Child Abuse or Neglect, or
(vi): to prospective adoptive parents upon initiation of adoption proceedings.
(b): An FSCW shall be authorized to recommend targeted financial and material assistance to parents, according to criteria to be developed by the Administration.
(i): An FSCW shall be authorized to predicate the receipt of such assistance on the parent’s participation in CPSMs, if the parent is not already participating in them.
(ii): The FSCW shall assist the parent, with substantial deference to parental autonomy, in self-monitoring parental choices, considering how well or poorly those choices serve the child’s welfare, and contemplating alternatives that might serve the child’s welfare better. The FSCW will be trained to be a parental resource rather than an imposing authority in this process.
(4): If either the FSCW or CF determine that a child is not in imminent physical danger but that the
child’s long-term welfare is being substantially compromised (according to the definition of Abuse or Neglect defined in 20-8-140 of the SHF Revised Statutes) by the child’s current home environment, (a): the parent can voluntarily submit to a process of Intensive Community Intervention (ICI), or
(b): the Administration shall investigate and determine if, by a preponderance of the evidence, the Administration’s determination accords with that of the FSCW or CF.
(i): If the Administration finds by a preponderance of the evidence that the child’s long-term welfare is being substantially compromised, the Administration shall initiate ICI.
(ii): If the Administration does not find that the child’s long-term welfare is being substantially compromised, then all adult parties will be brought together for a determination of how to proceed, which might include reassigning the parent to a different community, reassigning a new FSCW to the parent, or, if the parent prefers, maintaining the current FSCW and Community (and thus CF).
(c): Intensive Community Intervention (ICI) requires the voluntary involvement of Community and extended family members, as well as of teachers and others involved in the child’s life, working with the parent to rectify and remedy the problems that have been identified as substantially compromising the child’s long-term welfare. ICI strategies always include the determination of a designated period after which the case will be reviewed, and can include any combination of the following:
(i): parental behavior modification efforts, closely monitored by Community and extended family members, utilizing whatever institutional assistance is required (such as drug rehabilitation programs),
(ii): temporary in-home residence of Community or extended family member to assist the parent,
(iii): temporary placement of the child with a Community or extended family member,
(iv): limited or monitored parental contact with the child, and/or
(v): professional assistance in concert with the Community and extended family assistance.
(5): If as the result of an investigation into allegations of child abuse or neglect, or if an FSCW or CF determines that a child is in imminent physical danger; or if, after the designated period for an ICI, both the FSCW and CF determine that the ICI has been unsuccessful; or if an ICI was impossible due to a lack of willing extended family or Community members, the Administration will initiate a child custody hearing, adhering to the following guidelines:
(a): The Administration must find, by clear and convincing evidence, that the child’s long-term welfare is being substantially compromised, or that the child is in imminent physical danger, before parental rights can be wholly or partially terminated.
(b): The value of affective bonds and remaining in the child’s familiar home shall be given full weight as important, but not entirely decisive, factors in consideration of the child’s custody arrangements.
(c): Parental rights shall be terminated or limited only to the extent necessary to preserve the child’s safety and to secure the child’s long-term welfare.
(i): This Act imposes no presumption concerning the number of people that may be granted parental rights regarding a particular child, nor the precise scope of such rights in any given instance.
(ii): Preference will always be given to preserving and encouraging established healthy affective bonds between adults and the child, rather than severing such bonds in pursuit of parental exclusivity.
(iii): Partial, delineated parental rights may be granted to various adults, who must devise decision making guidelines commensurate with their various parental rights, with the assistance of an FSCW.
(iv): The Administration shall generate guidelines for relinquishing the rights and responsibilities associated with partial parental rights commensurate with the extent of those rights and responsibilities, and in accord with the child’s best interest, ensuring continuity of comprehensive parental services.
(v): “Parent,” for the purposes of this statute, does not refer to anyone with limited parental rights, but only to those with primary custodial rights, to be fully defined by the Administration.
(d): Consideration of custodial alternatives shall be given concurrently with consideration of the parent’s, and others’, custodial rights.
(i): The termination or diminution of parental rights do not necessarily result in an immediate or eventual loss of physical custody: The child will always be placed in the best available home, all factors considered, even if parental rights have been revoked from, or not yet granted to, the adult in whose custody the child is placed.
(ii): Preference will be given, in order, to (1) extended family members who are also members of the same Community as the parent, (2) other Community members, and (3) other extended family members, in any change of custody of the child, whether it is a temporary arrangement, the placement of the child in a foster home, or an adoption proceeding. The Administration has the authority to supersede or alter the ranking of these preferences in accord with particular circumstances.
(iii): No racial preferences beyond those implicit in the preferences above shall be implemented.
(iv): If the child can not be placed in a home according to the above preferences, and the Administration determines, by clear and convincing evidence, that the child’s safety or welfare is too drastically compromised in his/her current home to leave him/her there, the child will be placed in foster care and adoptive parents will be sought, with the parent retaining those rights of visitation, if any, that the Administration finds contribute to rather than detract from the child’s long-term welfare.
(e): Prospective adoptive parents must be members of a Community for one year prior to adoption, and must be recommended by their FSCW and the CF of the Community, and by a majority vote of both the community to which they belong and the Community from which the child is being adopted.
(f): A mother may not put her child up for adoption until 36 hours after the birth of the child if the decision was made in writing at least two months prior to birth, or three weeks after the birth of the child if the decision was not made in writing at least two months prior to the birth of the child.
(6): Extended family members, as defined in subsection (a), have the right to maintain a relationship with the child, subject only to the limitations delineated in subsection (b).
(a): An extended family member is, for the purposes of this statute,
(i): any blood relative of any parent (as defined in section 2 of this Act) that the child has ever had, who has formed a healthy affective bond with the child, as determined by clear and convincing evidence, according to criteria to be delineated by the Administration,
(ii): any other individual who, in a relationship sanctioned by any parent (as defined in section 2 of this Act), has formed a healthy affective bond with the child, as determined by clear and convincing evidence, according to criteria to be delineated by the Administration.
(b): The legal rights of extended family members (as defined in subsection (a)) to access to the child are limited in the following ways:
(i): No parent shall ever be obligated to relinquish temporary physical custody of a child to any current non-parent, unless by a formal hearing of the Administration the non-parent’s ability to have occasional temporary physical custody of the child, as opposed to mere visitation rights with parental supervision, is held, by clear and convincing evidence, to be vital and indispensable to the child’s long-term welfare, though the parent can rebut this finding by demonstrating by a preponderance of the evidence that any occasional relinquishment of temporary custody to the petitioning non-parent would be contrary to the child’s long-term welfare. If a finding in favor of the petitioning non-parent is made, the amount of occasional temporary physical custody shall be limited to the least possible to satisfy the needs of the child’s long-term welfare. The parent has the right of appeal; the non-parent has no right of appeal.
(ii): Non-parents with rights of access to a child are required to exercise reasonable self-restraint regarding the amount of access they demand, the degree of inconvenience they impose on the parent and other family members, and any disruptions or tensions that their relationship with the child may cause to or among the parent, family, or child. The Administration shall draft explicit guidelines regarding these issues.
(iii): Non-parents with rights of access to a child, who do not belong to the parent’s Community, shall be required to attend the Community Parent Support Meetings (CPSMs) at a frequency to be determined by the Administration, taking into consideration all relevant factors, though the frequency required may not be more than once per month nor less than once per year.
(iv): The parent can file complaints regarding non-parents with rights of access to the child, which the Administration is obligated to investigate, preliminarily through the agency of the child’s FSCW and CF. If the problem cannot be resolved to the satisfaction of all parties through the agency of the FSCW, CF, and CPSMs, a hearing must be held to determine if, by a preponderance of the evidence, the non-parent has abused his/her right of access to the child according to the criteria established by the Administration. If such a finding is made, then the non-parent shall have his/her right of access to the child revoked. Neither the parent nor the non-parent has the right of appeal regarding the determination of the Administration.
(20-8-140, a fictional statute to which I have cross-referenced in this hypothetical statute, would include conventional definitions of Abuse and Neglect, plus extreme emotional abuse).
I. Social Policy Concerns Addressed by the Act
This Act addresses the care and custody of children, including the rights and responsibilities of extended family and community members involved in a child’s life, the procedures for identifying and responding to child abuse and neglect, and the procedures for reassigning legal custody of a child. The purpose of this Act and the responsibility of the Administration is to facilitate communities and families in providing healthy and stable homes for children by means of mutual support, encouragement, involvement, oversight, and, in the last resort, reassignment of a child’s custodial arrangements, among family and community care givers. It is based on the principle that the state should be a proactive agent and vehicle of the people, to be utilized in conjunction with other social institutions in the facilitation of the welfare of its residents, rather than a reactive intervener of last resort, standing aside to permit preventable failure and subsequent suffering, and only then stepping in to pick up the pieces at greater public expense and with less efficacy.
This Act accordingly reconceptualizes the state’s role, relinquishing its theoretical commitment to initial minimal intrusion on family autonomy until a threshold is reached triggering a sudden extreme and generally inefficacious intervention (see Clare Huntington, “Mutual Dependence in Child Welfare,” 82 Notre Dame L. Rev. 2007, 1485: 1497-1505), and, in its place, constructing a state-family-community system which institutionalizes support to families prior to, and in prevention of, the failure of a family to provide for a child’s welfare.
The Act is characterized by two essential innovations: 1) a legal construct called “Community,” which mediates, buffers, and articulates the primarily coincidental and only marginally or superficially conflicting real interests of parent, child, and state; and 2) a proactive rather than reactive approach to child welfare policy. The Act meets the challenge of reconstructing and refining, through legal artifice, a traditional and organically produced social institutional form (i.e., community) that has grown increasingly attenuated with the growth of modern individualism, while not violating the Constitutional 14th Amendment liberty interests of parents (and others) which give that cultural individualism legal teeth. It does so in order to meet the corresponding political and legal challenge of increasing the constant and constructive involvement of the state in family and community life in order to decrease the extreme and often destructive involvement made more frequently necessary by its absence (or less comprehensive and humanized presence).
The central innovation of this Act is the introduction of the legal reincarnation of the Community, which serves, with focused intentionality in its new form as a legal construct, to mediate the tensions and alliances among the interests of parent, child, and state, and as a buffer coordinating the functions of family and state in more cooperative and mutually accommodating ways. It provides an arena of support, communication, negotiation, and resolution. It is a medium of both state coercion and parental resistance, the conflict between the two channeled, filtered, or dissipated according to the moderating, focusing, or amplifying influence of a middle-range of social organization through which both the individual wills of parents and the corporate will of society, via the agency of the state, must pass. It provides a familiar and intimate zone in which children have an increased opportunity to formulate and express their will, in which subcultural diversity can hold out against an often overreaching and categorically biased state demand for conformity, but in which authentic child abuse and neglect has reduced opportunity to hide. While no law or institution can either eliminate child abuse and neglect or erase all errors of overcontrol or undercontrol, of false positives and false negatives, the Community is designed to lower the rate of both child abuse and neglect itself and of errors in detecting it at both extremes, and to coordinate the freedom of parents to raise their children as they see fit with the desire of the state to ensure that those children are raised in a safe, healthy, and nurturing home.
The Community, as defined in this Act, 1) humanizes the state, 2) provides parents with improved due process protections, 3) channels information to the state to assist in accurate administrative decision making, 4) accommodates and protects diverse practices, 5) reduces institutionalized bias on the basis of race, ethnicity, English language proficiency, or social class, 6) mobilizes and moderates local normative control in service to child and family welfare, 7) channels relevant information and guidance to parents to improve parental decision-making, 8) facilitates continuity without sacrificing flexibility, 9) preserves and fosters rather than severs healthy affective bonds, 10) provides a buffer for strained relationships among adults involved in a child’s life, 11) provides a vehicle for including the child in the process, and, most fundamentally, 12) provides a vehicle of proactive state support of parents and families instead of state reaction to structurally-facilitated family failure.
The Community, as the humanized incarnation of the state, helps reduce the error of overly mechanistic or politicized responses by bureaucracies often processing children rather than attending to their needs, by relying instead on an intervening layer of intimate social bonds through which the state’s decision-making must operate. The current dysfunctions are poignantly illustrated in The Lost Children of Wilder (Nina Bernstein, 2001), from the institutionalized brutality of the Hudson Training School for Girls (pp. 8-26), to the institutionalized racism resulting from farming out child welfare services to private religious organizations (pp. 44-45), and on through the stories of bureaucratic in-fighting, severed ties, and inadequate mechanisms for adapting available human resources to children’s emotional needs. The need to humanize the process, to mobilize the many people of good will who would take an interest in the welfare of the children in their community were there a functioning community through which to exercise that good will, and to facilitate their ability to do so in concert and through mutual support rather than in mutual isolation, is eloquently argued both by the anecdotal evidence of current bureaucratic dysfunction (see Wilder; Elizabeth Bartholet, Nobody’s Children: Abuse and Neglect, Foster Drift, and the Adoption Alternative, pp. 8-15), and historical analyses of how our child welfare system became a vehicle of often punitive race, class, and gender bias through paternalistic and ethnocentric assumptions about the duty of the state and the incompetence of the people perceived to be (and often in reality) most in need of its services (see, e.g., Jill Elaine Hasday, “Parenthood Divided: A Legal History of the Bifurcated Law of Parental Relations,” Geo. L.J. 90: 299; Linda Gordon, Heroes of Their Own Lives: The Politics and History of Family Violence, Viking: 1988; Annette R. Appell, “Protecting Children of Punishing Mothers: Gender, Race, and Class in the Child Protection System,” 48 S.C.L. Rev. 577 (1997)). The viability of alternative, community-mediated, and family empowering approaches, on the other hand, is illustrated by the anecdotal evidence of successful historical and contemporary examples (see e.g., Dorothy E. Roberts, “Black Club Women and Child Welfare Lessons for Modern Reform,” 32 Fla. St. U. L. Rev. 957, 2005; Huntington, 1531-36 (discussing state-sponsored family-service programs that, while not specifically community-mediated, reflect the kinds of services that community mediation can most effectively deliver)).
Parental due process protections are improved as a result of this humanizing process by providing parents with a social resource through which their story can be effectively told. The Supreme Court, in Santosky v. Kramer, identified some of the structural challenges to the adequate provision of due process to parents in TPR proceedings, such as the state’s far superior ability to mount a case than the parents’ ability to mount a defense, and the conceptual separation of concern for the child’s welfare from concern for the parents’ due process rights (455 U.S. 745 (1982): 1310-11). In Lassiter v. Dept. of Soc. Servs., the Court accorded the loss of parental rights less due process than the loss of liberty, holding the former not to merit the requirement of appointed counsel (452 U.S. 18 (1981)). The Community, professionally organized and represented by the Community Facilitator, serves to mitigate these deficits by acting as a mediator, counselor, and conduit of information (sec. 2(b)(iv)). The resource thus provided helps to avoid what the dissent in Lassiter accurately identified as the average parent’s dilemma when opposed by the state in a legal proceeding: An inability to negotiate the rules and procedures of the court, resulting in an inability to mount an effective defense, coupled by, as in Ms. Lassiter’s case, what may well be a tendency for such lay people in such situations to exacerbate the judge due to their inability to follow the procedures expected of a litigant in court (pp. 62-60).
This by-product of an institution (the Community) serving multiple other purposes, incidentally increasing due process protection to parents in TPR proceedings, fares well under the scrutiny of the Mathews v. Eldridge test (424 U.S. 319, 335 (1976)): The Supreme Court has made clear that the parental interest in their parental rights is of the highest order of magnitude (see, e.g., Lassiter (1981), Santosky (1982), and Troxel v. Granville 120 S.Ct. 2054 (2000)); the state’s interest in keeping children with fit parents coincides rather than conflicts with this interest, while the state’s interest in efficiency is served by the multi-functional quality of the Community (including the more family-supportive roles of the professionals involved) by which parental due process is increased; and, finally, the benefits of this additional procedural resource in avoiding error is substantial. A corollary of this increased due process protection to parents is an increased flow of relevant information to the state, both to the Administration and the courts, thus resulting in the reduction of error discussed above. The benefits emanating from this one institutional innovation are widespread: Error is reduced not just in a single court proceeding, but in all administrative and legal action involving child welfare and parental rights.
The additional due process protections accorded to parents through the medium of the Community are substantive as well as procedural: The Community protects sub-cultural diversity and forms a bulwark against class, race, and cultural prejudices operating through the apparatus of the state. By providing people the opportunity to belong to a cultural (rather than geographical) Community if the choose (secs. 2(b)(i), (iii)), they are given an opportunity to preserve and insulate culturally divergent customs and practices. While the state still has a presence, and (what the state deems to be) unambiguously harmful practices will be prohibited, people with divergent customs are given a greater opportunity to preserve them in this Act than they would have in its absence (see sec. 2(b)(iii)). Furthermore, just as the Community protects divergent sub-cultures from the excesses of the conformity-imposing tendencies of the state, it protects historical victims of discrimination from the prejudicial presumptions of poorly informed state actors by embedding state actors in the Community with which they will be interacting.
The Community is an arena where compromise can be achieved: If Somali refugees wish to retain a symbolic remnant of female genital mutilation that does not inflict the physical harm of the actual practice (see “Refugees’ Beliefs Don’t Travel Well,” Chicago Tribune, Oct. 28, 1996), then, despite our cultural outrage at the symbolism itself, that can and should be accommodated. If it is Afghani custom for loving parents otherwise providing appropriate care to kiss, as a sign of affection rather than an expression of sexual intent, the penis of one’s child (see State of Maine v. Kargar (Maine S.Ct. 1996)), then a well-informed state might wisely choose to prioritize substance over form.
Of course, prioritizing substance over form does not always favor the divergent cultural practice. The Administration, if not the courts, might choose not to privilege spanking children with a ping-pong paddle for two hours in accord with the practices of a fundamentalist religious sect (see In Re Marriage of Hadeen, 619 P.2d 374: 620 (Wash. App. 1980)). Nor would it be incumbent on the state to permit parents to allow their children to die in lieu of providing medical care due to membership in the Christian Science church (see Hermanson v. State of Florida (Fl. S.Ct. 1992)). To the extent that federal law and the Constitution would allow, the Community replaces all other forms of deference to the particular, neither allowing it to justify what would otherwise be considered a clear and unambiguous infliction of substantial and palpable harm, nor forcing it to accede to vague and suppositional mainstream sensibilities. The issue remains the child’s welfare: Religion and culture can not excuse outright violence to the child, nor should the ethnocentrisms that seep through the state deny a family the discretion to provide a loving and safe household in accord with its customs and beliefs.
The Community reduces the salience of racial and class biases in three primary ways. First, it empowers the members of the sub-group, providing a bulwark against marginalization. The “othering” of poor families of color that Appell identifies (1997, p. 579) can not so easily occur when the “other” is not, in a sense, “divided and conquered.” When represented and expressed by a Community that is the overlap of “state” and “family,” the “other” becomes internalized, recognized, acknowledged, and, to some extent, accommodated. The norms are negotiated in that arena, not defined and imposed from without. Similarly, the frequently encountered language and cultural barriers Appell describes (Annette Appell, “Spanish-Speaking Caregiver,” 7 Nev. L.J. (2007)) are mitigated by the medium of a Community that acts as a linguistic as well as cultural translator. Furthermore, the thus-far prevalent cultural assumption is reversed: Instead of depriving a loving caregiver of her granddaughter on the basis of the erroneous assumption that she would be carrying the burden alone (see id., pp. 116-17), a Community both reinforces and raises the profile of extended family and community care-giving.
Second, the Community reduces the differential visibility of families of different socioeconomic classes (see Appell 1997, p. 584) by creating a continuous, recurring public interface for far more families regardless of socioeconomic class, an interface whose primary purpose is to ensure the welfare of the children in the Community. To a large extent, it merges together what Appell (1997, p. 581) identified as the bifurcated branches of public and private family law, one based on more intrusive treatment of the poor associated with child welfare intervention and the other based on more deferential treatment of the rich associated with property rights adjudication (see secs. 5(c), (d) of the Act). While it may be the case that more affluent than poor families opt for a Parental State-Disengagement Determination rather than belong to a Community, it is likely that many affluent families will be attracted to the material and social benefits of Community membership, and that the normative control (discussed below) exerted by Communities on its members will have an ameliorative effect across classes. Even those families that opt for a PSDD will have at least one encounter with the state in which their parenting skills and inclinations come under close scrutiny (sec. 2(d)), which may be one more encounter than they otherwise would have had.
Third, the Community, and complementary legislation (see sec. 2(b)(iv)(I)), reduce the rate of neglect-due-to-poverty by providing material, informational, emotional, and social support according to need, thus mitigating what Appell (1997, p. 585) identifies as the breach of white middle-class norms of proper child care that accompanies poverty. This channeling of resources and services in proactive support of families produces many benefits, just one of which is the reduction of class bias in our child welfare system. (Other benefits are discussed below.)
Like traditional communities before it, the Community will undoubtedly function as a vehicle of local normative control through the mutual enforcement of informal rules. This is accomplished by means of the diffuse social approval and disapproval of its members (see class, Jan. 27). The combination of the state’s involvement in the Community (see sec. 2(b)(iv)), and the historical tendency of communities in general to reinforce behaviors that are conducive to children’s welfare, are sufficient to ensure that the Community’s norms do indeed invoke positive and negative reinforcement of parental behaviors that, respectively, positively and negatively affect children’s welfare. In fact, due to the institutionalized interdependence Community members (see secs. 2(a)-(c), 4(b)), the externalities of individual parental choices is increased, and the incentive for other Community members to encourage good parenting and discourage bad parenting (as defined by some articulation of state and Community values) is correspondingly increased.
Indeed, the most likely, and perhaps most legitimate, criticism that may be leveled against this Act is that the Community itself can be a very onerous intrusion on family autonomy and privacy. But, aside from the opt-out provided by the PSDD, the tyranny of the Community is, if not necessarily reduced, then at least made more coextensive with individual freedom, by allowing parents the option of selecting a cultural Community that best expresses their individuality (see 2(b)(i), (iii)). Leaving aside for now the discussion of how the Act moves from, as Huntington put it, the somewhat mythological “freedom from” notion of family autonomy to a self-determination-increasing positive mutual engagement model (2007, pp. 1510-20), and considering instead the residual need of the state to intervene in remaining child abuse and neglect cases, the Community provides an appropriate balance between a family’s right to privacy on the one hand, and the state’s need to be vigilant in the protection of children’s welfare on the other. Deficiencies fostered by our current social institutional framework, such as the very inadequate job we currently do of identifying and intervening in cases of sexual abuse (class, Jan. 15), and the decreased ability to intervene in cases of child abuse and neglect in affluent households due to their decreased interaction with public services (see Appell 1997, p. 584), can be addressed more effectively, with a moderate and reasonable compromise of privacy, by means of a Community to which each family belongs, and under whose intimate vigilance each family thrives.
Along with the encouragement of practices conducive to child welfare and discouragement of practices antithetical to child welfare, the Community provides a conduit of information and guidance to parents to help them become familiar and comfortable with positive child care practices, as well as with coping skills to help avoid spontaneous responses to events that would be considered abusive or counterproductive to the child’s welfare. The Community Parenting Support Meetings (sec. 2) are, essentially, self-help group meetings held at regular intervals for just this purpose, as well as to resolve problems and address needs of individual families as they arise. As Huntington points out, this type of proactive assistance increases rather than decreases family self-determination, by “reducing the chance that a crisis will occur and the state will remove the child from the parent’s home” (2007, pp. 1511-12).
The reliance on the Community as the arena in which both proactive and reactive needs are addressed first, and are addressed most, balances permanence in the provision of a home for a child with flexibility in meeting the demands of ensuring that the home is a safe and nurturing one, and that all adults who have healthy affective bonds with the child are allowed to remain in that child’s life. As Bernstein explained in The Lost Children of Wilder, citing Bolby’s Attachment and Loss to explain Lamont’s traumatization by the shuffling around he experienced in the New York child welfare system, young children experiencing repeated cycles of attachment to adult care givers and subsequent loss develop reactions of anger and anxiety in association with the prospect of future attachments (2001, pp. 257-58). The Community provides an increased layer of the familiar around the family, facilitating the satisfaction of the sometimes conflicting demands of continuity on the one hand, and placement in a safe and healthy home on the other. It accomplishes this by 1) looking for foster care, adoption or temporary placement options within the Community first (secs. 5(c), (d)), 2) not severing the healthy affective bonds that the child has already formed in order to create parental exclusivity with each new placement (secs. 5, 6), and 3) investing in the proactive assistance to parents that will increase their ability to provide a healthy and safe home to their children in the first place (sec. 2(b)(iv)).
Our current child welfare system dramatically fails to meet these demands. Elizabeth Bartholet, in Nobody’s Children: Abuse and Neglect, Foster Drift, and the Adoption Alternative, identifies how the dysfunctional combination of excessive individualism and lack of community (p. 2), the notion of family autonomy as freedom from the state (p. 3), and “a powerful blood bias” (p. 7), creates a model which sets up often loving but poverty-impaired biological parents to fail and children subsequently to receive suboptimal care. According to Bartholet, child welfare services either leave abused or neglected children in the care of damaged parents deemed “good enough,” or place the child first in a sort of limbo awaiting the improbable event of the parent’s mostly unaided resolution of her problems, and then set the more-damaged-than necessary children adrift in a foster care system that is unlikely to provide either a stable or nurturing home (id., pp. 8-15).
Bartholet’s proposed solution involves the combination of a more proactive state assisting parents from pregnancy onward (id., pp. 15-16) and “concurrent planning,” “proceed[ing] on two tracks simultaneously, working with parents toward family reunification, while at the same time developing an appropriate adoption plan” (id., p. 18). The Community serves as a vehicle for a more comprehensive solution that incorporates Bartholet’s proposal, but also improves upon it. Not only does it provide a conduit for the state’s proactivity, but it does so with an inclusiveness and constancy that a mere patchwork of state assistance programs can not match. It facilitates blending concurrent planning with a focus on continuity for the child, by involving prospective adoptive parents in the child’s community from the earliest possible date (see secs. 2, 2(a), 5(e)), and by not forcing, as a matter of policy rather than as the result of an individualized determination, either prospective adoptive parents or biological parents (or any other care giver) to severe their ties with the child if the child ends up in the care of another (see secs. 5(b)-(d)).
This latter characteristic of the Act, of preserving rather than severing the healthy affective bonds that children have formed with adults (secs. 5(c), (d), 6), contributes not only to continuity for the child, avoiding the attachment-interruption problems described above, but also provides the child with increased adult human resources on which to draw. Who could doubt that, had Alicia’s loving bond to Lamont not been arbitrarily severed (see Bernstein, pp 300-302), had care instead been taken to preserve it, that Lamont would not have fared better? Or, for that matter, had Shirley been able to maintain some kind of relationship with Lamont throughout his childhood, even if not a custodial one, that they both would not have benefited (id.)? The Act explicitly allows for any number of adults to be involved in a child’s life, to have plenary or circumscribed roles, responsibilities, and rights, and for those roles, responsibilities, and rights to be coordinated in mutually accommodating ways by the Community and the agents of the Administration (secs. 5, 6). Through these mechanisms, the Act addresses and mitigates many of the problems associated with allowing more than two parents, while retaining all of the benefits (see class, March 5).
The literature is rife with examples of severed or attenuated bonds between children in the system and adults who love them, often followed by disastrous outcomes for the child (or simply the loss of a loving parental figure) (see, e.g., Apell 1997, pp. 592-93; Appell 2007, pp. 116-21; Bernstein 2001; Suzanne Goldberg, “Family Law Cases as Law Reform Litigation,” 17:3 Colum. J. Gender & L. 307, 2008). The case law also provides numerous examples of the exclusion of adults who wished to form a relationship with the child, frequently on the basis of parental exclusivity (that is, only two parents per child) (see, e.g., Quillon v. Walcott, 434 U.S. 246, 1978; Michael H. v. Gerald D., 91 U.S. 110, 1989; Sider v. Sider, 334 Md. 512, 1994; In Re Baby M., 109 N.J. 396, 1988; Ohr v. Ohr, 97 P.3d 354, 2004; In the Interest of CTG, 179 P.3d 213, 2007). While in some individual cases a determination might be reached that a particular relationship is not in the child’s best interest, the presumption that a child can have no more than two adults with parental or quasi-parental rights severs valuable bonds and reduces the affective human resources available to the child.
The focus on fostering and preserving healthy affective relationships with adults, and contextualizing the child’s welfare by membership in a Community, provides resources that can also serve as a buffer when necessary between two adults with shared parental rights. In In Re the Paternity of Baby Doe (207 Wis. 2d. 390, 1996), the court held that, absent a statutory distinction, the rapist father of a child had the same rights as any biological father. If, even under a more refined legislative regime, a rapist-father’s relationship with the child were found under certain circumstances to be in the child’s interest, the presence of multiple adults in the child’s life, and of a Community enveloping those relationships, could more easily accommodate a mother who might well be highly averse to any kind of interaction with the father. Even under less dramatic circumstances of divorced parents highly antagonistic to one another, the best solution at times, if all else fails, might be to preserve the child’s relationship with each while sparing all from forcing a relationship on the two antagonistic adults. Moving away from the current insular family microcosm and toward a Community model of socially contextualized families would facilitate such flexibility.
The Community, as a facilitated organic medium for, among other things, interpreting, coordinating and accommodating the wills of various actors vis-a-vis the children whose welfare is the purpose of this Act, is able to give voice to those actors whose voice is most marginalized, though whose interests are most pertinent: the children themselves (see sec. 2(b)(iv)(III)). Just as the Community can interpret for care givers who are not fluent in English, it can interpret to some extent for children whose cognitive development renders their conceptual language to some degree out of sinc with the conceptual language of the adults around them. This is a function of the combined genius of numbers and of intimacy: The more intimate one is with a child, the more that adult can intuit the child’s thoughts, wishes, and perceptions; and the more adults so positioned, interacting both with each other and with the child over extended periods of time, the more able they are collectively to extract and render comprehensible the perceptions and wishes of that child.
Children’s participation in Community Parenting Support Meetings, and their interaction with the Community Facilitator and with their family’s Family Support Case Worker (if they have one), will help to empower the children, and teach them through experience not only civic participation, but also how to live in a community, how to advocate for themselves, and how to engage with the world in a more aware and proactive way. The skills they thus actively develop, as well as the institutional apparatus through which they develop it, will help mitigate some of the inherent and, to varying degrees, intractable challenges facing the extension of rights of self-determination to children.
As Justice Douglas put it in his dissent in Wisconsin v. Yoder, “the children should be entitled to be heard” (406 U.S. 205, 241: 244 (1972)). In Yoder, the rights of the parents, the state, and even of the reified Amish religion and community, were all considered, but the children were the ball rather than the players moving it down the field (see class, Jan. 29, though the metaphor is mine). The difficulty of obtaining a fully informed and well articulated statement from children involved in matters of concern to them, and the question of how to weigh such statements if obtained given the children’s cognitive limits (id.), contribute to the marginalization of a child’s will in determinations of that child’s fate.
Perhaps most saliently, how could the state enforce a child’s right vis-a-vis a fit parent, when that child remains dependent on that parent (class, Feb. 3)? One step toward resolving these challenges is to provide the child with a social resource that is neither the parent nor the state, that is familiar with and supportive of the child, that is not an individual either guessing at the child’s best interest (e.g, a guardian ad litum) or a lawyer representing the child’s uninterpreted express views and preferences (see Elizabeth Brodsky’s class presentation on April 21), but is rather a Community that knows the child and can help the child to discover, formulate, and articulate his or her own views and preferences most effectively. And, perhaps most uniquely and importantly, the Community reduces the child’s absolute dependence on the parents with whom he or she is identifying imperfectly aligned interests.
The parental advantage is far from eliminated in this context: The Community is always of the parent’s choosing (unless accepted by default). In Yoder, the relevant Community (the Amish community) would have sided unambiguously with the parents. The children would have had to leave their Community as well as their families to escape the adult will to which they were being subjected. But the Community will provide many children in many situations with an adult social resource that is more attuned to them then a GAL is likely to be, and is capable of being the child’s most powerful advocate in certain circumstances. And the presence of state actors in the Community (the Community Facilitator assigned to the Community itself, and the Family Support Case Workers assigned to families within the Community) helps to provide at least some counterweight to the Community’s own potentially totalitarian inclinations.
Those totalitarian inclinations pose a serious challenge. The Community can as easily be the oppressor as the liberator, an increased weight dictating to the child (or parents) rather than an asset supporting them. Care must be taken in the design and management of Communities to prevent them from becoming suffocating forces, and to maximize their potential as an empowering resource.
In many ways, the Community’s ability to perform effectively its functions is due to it being a permanent and familiar presence rather than a foreign agent suddenly introduced in response to events. And this, of course, is the crux of its utility: It is the vehicle of a proactive rather than reactive approach to the provision of child and family welfare services. The Community is the comprehensive operationalization (and marginal refinement) of Huntington’s “‘engagement with’ model of family-state relations,” which replaces “the ‘freedom from’ conception of family autonomy” (2007, p. 1485). Like the African-American child and family welfare advocates at the turn of the 19th to 20th centuries (Roberts 2005), this model is focused on supporting rather than penalizing parents and families facing the challenges of providing for their children, and particularly those families that are further burdened by the deprivations of poverty (Huntington 2007, p. 1494).
Following Barbara Bennett Whitehouse’s (Ecogenerism: An Environmental Approach to Protecting Endangered Children, 12 Va, J, Soc. Pol’y & L. 409, 423 (2005), cited in Huntington 2007, p. 1496) identification of the salience of a child’s environment, “including a child’s peer group, neighborhood, and school” as “the systems surrounding a family” that should be supported in conjunction with the support of the family itself (Huntington, p. 1496), the Community is the vehicle for directing that support and coordinating the various components of a child’s environment. And rather than providing the “one-way ratchet” effect of regulation-imposing state aid (Huntington, p. 1506), the Community provides a two-way forum of state and family articulation.
As Huntington points out (citing Frances Olsen, “The Myth of State Intervention in the Family, 19 U. Mich J.L. Reform 835 (1995)), the state is already heavily implicated in family decisions, first by “determin[ing] the contours of the world in which a family lives,” and second by “establish[ing] a system authorizing parents to make some decisions concerning children” (Huntington, p. 1514). In essence, the illusion of family autonomy is a function of the degree to which we accept the state’s involvement as a fixture of the social institutional environment, and so do not identify it as state involvement at all. Public education, for instance, is an enormous state investment in our children’s development (Huntington, p. 1522), one that affects children’s development in an often cooperative and occasionally conflicting dialectic with individual families (or, indeed, individual communities), but one that is not generally perceived as an unacceptable intrusion on family autonomy. Indeed, most parents have come to see it as an indispensable state service.
There is no inherent, qualitative difference between the institution of public education, which parents generally accept and appreciate, and the institution of the Community established by this Act, which families could well come to accept and appreciate in much the same way. Just as the state has created an elaborate apparatus, both local and ubiquitous, to provide public education services, so too can it provide a similar apparatus, the corollary of the local school, providing comprehensive support to families in the enterprise of raising their children. And just as public education is an enormous investment that has paid off enormously, the fully endowed Community (see sec. 2(b)(iv)) holds the same promise multiplied many fold.
The Community as a legal construct satisfies not only the need to provide a conduit through which to channel state services to families that need them, but also the need to replace, in some form, a valuable traditional social institution that has eroded with increased mobility and increased familial and individual insularity. The Yoder Court, by one not terribly strained interpretation, appears to have been implicitly informed by an appreciation of and deference to the stability and nurturing environment that a well-functioning community provides (406 U.S. 205 (1972)). The Community is the family writ large and the state in humanized form; it is the middle ground. As such, it provides many benefits beyond those that are the focus of this discussion, such as, by permitting and coordinating multiple adults participating in a child’s life, the facilitation of non-traditional family arrangements (see In Re Baby M 1988; John Bowe, “Gay Donor or Gay Day?” New York Times, Nov. 19, 2006).
The Community is also an improved social thermostat, responding in real time to evolving situations, rather than, as in our current child welfare regimes, relying on a remote state which must choose between removing a child from his or her home (and thus ensuring that he or she is at a statistical disadvantage of faring well (class, Jan. 22), as well as risking the outright abuse found within the foster care system (see Taylor v. Ledbetter, 11th Cir. 1987)), or, conversely, risking a catastrophe such as that illustrated by DeShaney v. Winnebago (7th Cir. 1989), in which a boy was not removed from an abusive home and, subsequently, was beaten into a coma by his father and suffered permanent brain damage as a result. The Community satisfies the risk-aversion of the state (class, Jan. 22) by being its more vigilant immediate presence, but simultaneously permits less precipitous removal of the child than is often the result of that very same risk aversion (see, e.g., Appell 2007, pp. 116-121; Bernstein 2001, pp. 189-97).
The Act contextualizes all decisions made regarding child welfare, and places all adults currently or prospectively involved in such decision-making (see, e.g., secs 2, 5(e), 6(b)(iii)) in the relevant Communities, aided by the trained professionals within those Communities. The professionals are attached to both levels (a CF for the Community as a whole, and FSCWs for individual families within the Community) in order to increase communication and cooperation across levels. Some flexibility for individual Communities and care givers is incorporated into the Act, such as, in sec. 2(c), allowing for some variance in the frequency of Community Parental Support Meetings, in sec. 2(c)(ii) allowing for accommodation of individual parents with scheduling problems, and in 6(b)(iii) allowing for variation in how frequently adults with more peripheral roles in a child’s life must attend meetings (depending on factors such as geographic distance). This flexibility combines assurance of actual integration into the Community with avoidance of making Community membership an onerous burden.
The use of the Community, with the oversight of the CF, to target resources to families in need (sec. 2(b)(iv)), increases the efficiency of the channeling of resources to where they are needed, and deferential assistance in most effectively utilizing those resources.
The Act strikes a balance between protecting privacy concerns and creating an intimate social context for proactively providing and targeting family services in provisions such as sec. 2(c), which provides parents with an opportunity to opt out of the entire proactive apparatus of the Act, after a deferential meeting to determine that there is no reason why the parent shouldn’t be allowed to do so. This meeting is designed to ensure that no parent remains completely insulated from the child welfare system created by the Act, and to give the Administration at least one chance to detect any obvious signs of concern before a parent is allowed to retreat into the current default of family insularity that is so conducive to undetected child abuse and neglect. Parents who do not opt-out can participate with varying degrees of engagement, receiving varying amounts of professional support, depending on a combination of their choices and the Community Facilitator’s recommendation (sec. 3).
Section 4 provides an escalating process of intervention when necessary for the child’s safety or welfare, beginning with Community support and guidance if at all possible. Due to liberty concerns, the Act cannot mandate that Community members provide that support and guidance, though the hope is that by institutionalizing the opportunity and providing a framework through which to operationalize Community support and guidance (absorbing the transaction costs, so to speak), such support will become the norm rather than the exception. Section 5 continues the provision of steps to be taken to remove a child from a dangerous or unhealthy home, always focused on creating the least disruption possible to the affective bonds that the child has formed with adults, and contemplating available alternatives simultaneously rather than sequentially (secs. 5(d), 5(d)(i)), thus avoiding terminating a bad situation in favor of a worse situation. The concerns for maintaining continuity of racial and sub- cultural identity for the child are incorporated into the preferences outlined in sec. 5(d)(ii), and neither merit nor require any additional privilege. Sec. 5(e) further facilitates continuity for the child in adoption proceedings, and increased assurance of a good fit, by involving the prospective adoptive parent in a Community as soon as adoption proceedings begin, and encouraging involvement in the child’s Community as soon as possible by requiring the Community’s approval of the adoption.
Section 5(f) is a slight modification and refinement of current (Colorado) rules of adoption requiring a four day waiting period after birth before a mother can put her child up for adoption (CRS sec. 19-5-103.5(1)(b)(IV)). Section 5(f) distinguishes between a considered decision made well before birth, and a precipitous decision made after birth. While sec. 5(f) recognizes the wisdom of giving every new mother a brief opportunity to reconsider her choice, it also recognizes that it is in the interest of mothers who made that choice rationally well prior to birth to abbreviate that period as much as possible (36 hours in this case), while for mothers who may be making the decision more precipitously it is important to extend that period enough (3 weeks in this case) to ensure that it is, in fact, a well-considered and rationally made decision.
While section 6 describes the provisions for fostering and maintaining healthy affective bonds with all adults actually involved in the child’s life, it also recognizes the parent’s ultimate responsibility and right to be vigilant regarding such relationships (sec. 6(b)(i)). Sections 6(b)(ii) and (iv) similarly protect the parent’s privacy vis-a-vis other adults with rights of access to the child, and address the logistics of ensuring that such rights are exercised in a minimally intrusive and disruptive way.
II. Constitutional Issues Raised by The Act
The Constitutional issues raised by this Act center on the 14th Amendment liberty interest of parents in their parental rights regarding the custody and care of their children, and the penumbra privacy right found through a distillation of the 1st, 3rd, 4th, 5th, and 9th Amendment rights. The case law at hand focuses on the 14th Amendment liberty interest, and, following that case law, I believe that the Act can withstand a 14th Amendment challenge. In Troxel v. Granville (120 S.Ct. 2054 (2000)), the Court, in a plurality decision, struck down a Washington statute permitting any person at any time to petition for child visitation rights against a parent’s express wishes, on the bases that the statute was overbroad, and that parents have a fundamental right protected by the due process clause of the 14th Amendment regarding the care and custody of their children. But the holding is ambiguous, in that the Court does not apply strict scrutiny despite the identification of a fundamental right (see J. Thomas’s concurrence, 2067-68). And the Court’s holding, “as applied” (p. 2060), strongly implies, if not explicitly states, that not any statute permitting people with specified relationships to the child to petition for visitation against parental will would not necessarily be unconstitutional according to this holding, but only a statute that permits “any third party seeking visitation to subject [a contrary parental decision] to state-court review” would be (p. 2061, emphasis mine). Since the Act (sec. 6) specifies that only adults that have formed healthy affective bonds with the child have such right of petition (and, had space allowed, would have made detailed provisions for biological parents who had not formed such bonds), it does not suffer the defect that caused the Washington statute in Troxel to be struck down.
Troxel only requires special deference to parents not found unfit, on the rebuttable presumption that parents have their child’s best interests at heart (pp. 2061-62). The Act above provides such deference. In sections 6(b)(i), (ii), and (iv) of the Act, the special deference accorded parents is codified in precise detail. Section 6(b)(i) ensures that the parent can always be present, if she chooses, in any visitation with her child by any other adult, unless a very high threshold is met to demonstrate that the child’s best interest is served, and no harm is threatened, by the non-parent’s ability to visit the child without the parent’s supervision. Sections 6(b)(ii) and (iv) specify the deference to parents required by non-parents exercising these rights, and the procedures available to parents who feel that appropriate deference (specified in the regulations) was not exercised.
The Supreme Court of Colorado, in In Re R.A. (137 P.3d 318, 2006), interpreting Troxel, construed the Colorado grandparent-visitation statute to contain a rebuttable presumption that parental determination is in a child’s best interest, the burden being on the grandparents to prove by clear and convincing evidence that it is not in the child’s best interest. The Act, by placing the state, as parens patriae (see class, April 16), in the position of the petitioner, in essence legislates precisely this proposition: In sections 6(a)(i) and (ii), petitioners for such third-party visitation rights must demonstrate to the Administration, by the same standard of proof as that identified by the Colorado Supreme Court (“clear and convincing evidence”), that they have already formed a healthy affective bond with the child, thus, if opposed by the parent, rebutting the presumption that favors the parent’s judgment.
The traditional two-parent limit, which this Act modifies, appears from the available sources to be an artifact of state statutory law rather than any form of federal law (whether Constitutional, statutory, or regulatory). The authority cited in Elisa B. (117 P.3d, 664) and Ohr (97 P.3d, 356) for the two-parent limit is the Uniform Parenting Act, as enacted by the states of California and Colorado, respectively. The Supreme Court of California weakly implied, in Elisa B. (117 P.3d, 665), that there is nothing to prohibit, a priori, a state from legislatively recognizing multiple parents, stating “we see no compelling reason to recognize [a multiple parent arrangement] here,” citing California law, and neither Constitutional nor federal law, as their authority. The Colorado Court of Appeals stated it more strongly in Ohr: “We think it best to leave to the General Assembly the decision whether to extend eligibility to seek parenting time…” (p. 358). The sharp distinction the courts consistently make, however, between “parents” and “third parties” (see, e.g., Troxel, p. 2061; Johnson v. Calvert 5 Cal.4th 84, cited in Elisa B, p. 665), raises some concerns that a diffusion of parental rights vis-a-vis a single child could confront a Constitutional challenge. However, since no provision in the Constitution speaks either directly or indirectly to this issue, one would hope that judicial restraint would prevail.
The remaining 14th Amendment question is whether the requirement of attending a Parental State-Disengagement Determination in order to opt-out of the family-state engagement (Community) provisions of the Act violates a parent’s liberty interest in the care and custody of her children. Using Huntington’s analogy of public education (p. 1522), and noting that there is no Constitutional prohibition to imposing procedural requirements on parents wishing to disengage from the state in regards to compulsory public education as onerous as, or more onerous than, those incorporated into this Act in order to disengage from the Community (see, e.g., Pierce v. Society of Sisters, S.Ct. 1925, holding that parents can remove their children from public schools only if they send them at their own expense to state-regulated private schools instead), there is no reason to believe that a Constitutional challenge to the requirement of meeting with the Administration one time in order to disengage from the arguably more invasive elements of this Act would be successful.
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!

Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
Accessing Intensive Mental Health Services (AIMS) for Children Report:
The Co-Occurring Disorder Dilemma
Written by Steve Harvey, Esq., J.D., M.A.,
Funded by a University of Colorado Law School Judicial Fellowship
Executive Summary:
This paper addresses the widely reported but poorly documented problems in the coordination of Medicaid services for children and adolescents with co-occurring conditions with behavioral implications, including mental illnesses, developmental disabilities, autism spectrum disorder, traumatic brain injury, and fetal alcohol syndrome.
Even though the behavioral services and treatments appropriate for these conditions are often identical, the structure of Colorado’s Medicaid program is such that families must qualify for help from different providers, using different eligibility criteria, often based on an arbitrary assessment of which behavioral problems are attributable to which diagnoses. The consensus among professionals in the field is that there is no diagnostic or clinical basis for this distinction. It is an administrative artifact that leads to onerous difficulties for already overburdened families seeking services, and the potential denial of services to children who are both eligible for them and would benefit from them.
There appears to be widespread recognition of this problem among professionals and other stakeholders in the Colorado behavioral health and developmental disabilities communities. Families experiencing such obstacles most frequently report that they occur through informal denials, rather than a formal Notice of Action (NOA) that can be appealed or aggrieved.
It is the recommendation of this report that the state conduct a comprehensive study to determine the extent of the problem, what best practices should be implemented, and, if appropriate, what changes can be made to better coordinate and integrate related behavioral health services.
Table of Contents
Section One: Introduction……………………………3
Statement of the Problem…….……………………..3
Basic Overview of Colorado Medicaid and Behavioral Health Services…….4
Section Two: Statement of the Goals of the Project………………6
Section Three: Anecdotal Evidence……………………………………6
Case Study One…………………………………………………….7
Case Study Two…………………………………………………….9
Case Study Three………………………………………………..10
Anecdotal Evidence of Informal Denials (or “Non-Denial Denials”)…11
Section Four: BHO Formal Denials Data……………….12
Section Five: An Analysis of Relevant Issues…………14
Section Six: An Example of a Program That Works Well (Intercept Center)…..22
Section Seven: Possible Solutions and Recommendations………23
An Overview of Policy Goals……………………………23
A Survey of Specific Solutions………………………26
Conclusion…………………………………………………29
Methodology…………………………………………30
Section One: Introduction.
Statement of the Problem.
This report addresses a widely recognized but poorly documented gap in the provision of mental health services to children and adolescents1 on Medicaid who have co-occurring conditions with behavioral implications (which I will refer to throughout the report as the “Co-Occurring Disorder Dilemma”). Children who exhibit behavioral problems consistent with a covered mental health diagnosis, who also have such co-occurring conditions as developmental disabilities (DD), autism spectrum disorder (ASD), traumatic brain injuries (TBI), or fetal alcohol syndrome, are sometimes, perhaps frequently, formally or informally denied the mental health services to which they would otherwise be entitled.
My primary task, initially, was to determine the frequency and causes of the Co-Occurring Disorder Dilemma, and whether it required a system-wide solution. Some of the reports received by those who informed me of this problem indicated excessive administrative barriers. Some indicated poorly trained in-take personnel and misinformation given to applicants as a result. In the course of researching and compiling the report, some of the underlying dynamics of the problem became clearer, and some strategies for improving access to covered Medicaid mental health services for multiple diagnosis children and adolescents began to emerge. These strategies, as discussed in detail in Section Seven below, involve identifying the different kinds of obstacles to access involved, how they interact, and the different kinds of institutional reforms that can address them.
Cases coming to the attention of advocates and attorneys, and discussions with advocates, attorneys, providers and parents who have dealt with similar problems raised concerns that this might be a chronic, critical structural problem in the Colorado Medicaid program. In order to assess how prevalent this problem was, I simultaneously sought out quantitative data and anecdotal evidence. As discussed in the Methodology section at the end of this report, the research involved talking with stakeholders, reviewing documents, and requesting data, which was then sorted, distilled, assembled, and compiled to form this report.
The most critical conclusion that can be drawn from the evidence assembled is that some families, already burdened in extraordinary ways with children whose behavioral problems are onerous and overwhelming (often accepting this responsibility voluntarily by adopting children that others would not), are left without recourse, without assistance, and often with only desperation and frustration. They encounter a system that, to them, seems to be comprised of walls without doors. The evidence also demonstrates that this is not necessary. It is not dictated by limited resources but rather by limited imagination and resolve. Significantly superior outcomes are well within reach, outcomes more conducive to the individual and family welfare of those most directly impacted, and to our collective fiscal, economic, and social well-being.
This report examines one set of systemic problems in how we manage and provide mental health services to Medicaid-eligible children and adolescents. Nothing in this report is intended as an indictment of any individual or any particular organization, even when a critical eye is cast at the institution they represent or the incentives they are confronted with. The goal is to create systems that ensure optimal performance (including ensuring that the system most effectively selects and incentivizes the individuals within it), regardless of the particular individuals occupying particular positions at any particular time. The purpose of this report, then, is to help inform actions dedicated to realizing institutional reforms that reduce or eliminate the Co-Occurring Disorder Dilemma.
Basic Overview of Colorado Medicaid and Behavioral Health Services.
Medicaid is a federal program administered by the states that opt to participate in it (which all 50 states do), and funded jointly by federal and state governments. The Early Prevention, Screening, Diagnosis and Treatment (EPSDT) program is “Medicaid for children.” It eliminates the distinction between mandatory services (those that states must provide) and optional services (those that states may provide but don’t have to), obligating states to provide all medically necessary mandatory and optional services for all child and adolescent Medicaid clients. It also mandates a series of screening, diagnostic, and treatment protocols to ensure a higher lever of intervention and care for children on Medicaid.
Colorado Medicaid, in compliance with federal law, is overseen by a single agency, the Colorado Department of Health Care Policy and Financing (HCPF). This agency is completely separate from the Colorado Department of Human Services (CDHS), and the Colorado Division of Behavioral Health (CDBH) within CDHS.
HCPF contracts with five regional Behavioral Health Organizations (BHOs) to manage the provision of behavioral health (i.e., mental health and substance abuse) services covered by Medicaid. The BHOs are paid a “capitated” rate, determined by the number of people on Medicaid in their region, their eligibility category, and the historical trends concerning costs per person. The services themselves are provided by Community Mental Health Centers (CMHCs) and provider networks that contract with the BHOs. This managed behavioral health care system is often referred to as “Capitated Medicaid.”
The five BHOs, seventeen CMHCs, and five specialty clinics are members of an umbrella nonprofit organization called The Colorado Behavioral Healthcare Council (CBHC). CBHC represents the interests of these members.
The BHOs are contractually obligated to manage the provision of medically necessary covered services (as outlined in Exhibit E of the state’s contract with the BHOs), that carry one of the covered procedure codes listed in Exhibit F of the contract, for one of the covered mental health diagnoses listed in Exhibit D of the contract, by a provider credentialed to provide that procedure for that diagnosis (as outlined in Exhibit O of the contract).2
Diagnoses, services, and procedures not listed in Exhibits D, E, and F of the state’s contract with the BHOs, but otherwise covered by Medicaid, are considered “medical” services, and are administered separately through a system by which providers bill the state for each procedure or service according to a predetermined billing schedule. This is called “fee-for-service” Medicaid. The four major co-occurring diagnoses (DD, ASD, TBI, and Fetal Alcohol Syndrome), and most services commonly associated with them that are covered by Medicaid, are covered under the fee-for-service system.
Twenty geographically defined Community Centered Boards (CCBs) are responsible for meeting the needs of individuals with developmental disabilities and developmental delays. Various advocacy organizations, advisory councils and committees, comprised of various kinds of stakeholders (including service providers, government agency officials, managed care CEOs/EDs, advocates, and “consumers”), intersect with and overlap the formal structure described above.
Section Two: Statement of the Goals of the Project.
The original purpose of this project was to look beyond the anecdotal evidence to determine the scope, intensity, causes, costs, and possible solutions of The Co-Occurring Disorder Dilemma. But research quickly revealed that a fundamental aspect of the dilemma is the degree to which relevant data is either not collected or not aggregated and analyzed, leaving little information other than anecdotal evidence available for consideration.
Due to the relative lack of data, the project has evolved. Anecdotal evidence of the nature of the problem remained an integral component. But, rather than attempting to quantify it, emphasis shifted to an analysis of the underlying dynamics and issues involved. This analysis helps to frame consideration of the range of possible solutions, including programs currently in existence that do a better than average job of attending to the needs of multiple diagnosis children. Denials data generously provided by the Behavioral Health Organizations (BHOs) are also summarized and discussed.
This report does not address several related issues. Among them are deficiencies in funding, deficiencies in covered diagnoses and treatments, deficiencies in the availability of providers or facilities, or hospital denials of in-patient care to multiply diagnosed children in crisis. It does, however, touch upon the issue of the adequacy of training for providers and in-take personnel, since this is a crucial component of The Co-Occurring Disorder Dilemma.
Section Three: Anecdotal Evidence
Among the parents, advocates, program directors, and service providers that I interviewed, there is a widespread and deeply felt perception of a serious and pervasive problem that needs to be addressed. At a stakeholder meeting held by the Colorado Department of Human Services (CDHS), there was repeated discussion of what I am now calling the Co-Occurring Disorder Dilemma by various stakeholders and a murmur of acknowledgement by other attendees whenever it was mentioned. While popular perception of a phenomenon does not prove its existence, popular perception by professionals of a problem relating to their profession is at least suggestive and warrants due attention.
Other than such perceptions, the principal evidence for the existence of the Co-Occurring Disorder Dilemma is comprised of the personal stories of those parents of multiple diagnosis children who have encountered it. A few of those stories are recounted below.
Case Study One.
C (child) was placed in P’s (parent’s) home when C was 6, having suffered severe abuse in his birth home. His birth family, for instance, had tried to “cure” his Tourette Syndrome by pouring caustic chemicals down his throat.
C had a low IQ and was at times very violent, flying into uncontrollable rages. In one instance, he broke both the hands of his disabled adoptive father and cut his (the father’s) face with broken shards of glass. He also frequently tried to hurt himself. When not suffering such an episode, however, he had a completely different personality, and would be overcome with remorse. This was a heavy burden for P and her husband, who undertook this responsibility that few others are willing to.
Despite this pattern of behavior, and his mental health diagnoses of mood disorder, PTSD, and OCD, his BHO never authorized residential services for C, even after episodes of extreme violence. The BHO said he wouldn’t benefit from behavioral health services, that his behavioral problems were a result of his developmental disability rather than his mental illness, and that the behavioral issues were the responsibility of the Community Centered Boards (which address developmental delay issues) rather than of the BHOs.
On three occasions, once for six weeks, P managed to access the Neuro-psychiatric Special Care (NSC) in-patient and day treatment services at Children’s Hospital, an excellent but overburdened treatment program for children with dual (or multiple) mental health and developmental disability diagnoses. NSC bills as a psychiatric treatment center under capitated Medicaid (requiring a mental illness diagnosis, as C had, and a BHO determination that the behavioral problems for which treatment is being sought is a result of the mental illness, as P had to advocate for). C had received medical services related to a suicide attempt, and, due to the bifurcated billing discussed below, could not access mental health services at the same time. While in the NSC center, follow-up surgery was required, but to get it, P would have had to have C discharged from the NSC unit and readmitted on the medical side, causing C to lose his place in the NSC unit and be placed on a six month waiting list to get back in.
According to P, her BHO had told her that since C was adopted, C was social service’s responsibility, but this is only true in dependency and neglect cases. When C was 12, social services placed him in the category of “at-risk youth” or “child out of control of parents,” adding their interventions to the burdens that P was facing. Thus one of the perennial problems of bringing in social services arose: P faced a threatened dependency and neglect determination. Having adopted a child with developmental disability and mental illness diagnoses, seriously abused in infancy, showing signs of PTSD and Reactive Detachment Disorder, desperately seeking appropriate care for this child, P found herself under a cloud of presumed suspicion.
During the course of this years-long ordeal, P had to use the emergency room as an alternative to the residential care that C needed, as is frequently reported in such cases. On one occasion, she had to wait in the emergency room until a bed opened up for C, bringing her husband and plugging his ventilator into a wall socket in the emergency room, and not going to the bathroom (which would have been considered “abandonment” of the child). After all that, C was not admitted because the BHO was called and refused to cover the expense.
As numerous service providers, advocates, and family members have noted, only the most tenacious parents, who advocate relentlessly for their children, generally succeed in cutting through these kinds of obstacles. For instance, it was a threat by P to file an American with Disabilities Act (ADA) Section 504 complaint that first got the BHO to the table after continually refusing to provide mental health services.
As a result of P’s tenacity, some progress was made on the DD (fee-for-service) side. C was placed on the wait list for the children’s extensive support (CES) waiver. The CES waiver is for DD children who need 24 hour line-of-sight care, and provides about $30,000 of services, in-home behavioral support and respite care. P’s CCB used local money for people on the wait list and provided in-home behavioral support. Eventually, the Colorado Cross Disability Coalition (CCDC) got everyone at the table to kick in something for in-home care, and talked about creating a virtual residential treatment center in the home. (C passed away due to complications related to his pre-adoption abuse before this could be implemented.)
Case Study Two.
Q (parent) adopted D (child) when D was two weeks old. There were immediate neurological symptoms. D was originally diagnosed with attachment disorder. Therapy helped a little.
D was later diagnosed with Schizophrenia, “mood disorder with psychotic features,” and ASD, and received a year of day treatment. Q believes that the behavioral issues need to be treated regardless of the diagnostic labels attached to them, but relies on the mental illness diagnoses to access necessary and appropriate mental health treatments for D.
Despite the Schizophrenia diagnosis, Q’s BHO refused to provide behavioral treatments appropriate to D’s mental illness diagnosis, stating that the BHO doesn’t provide services for Autism. Subsequently, Q used D’s Schizophrenia diagnosis to obtain treatment, without disclosing that D also had ASD.
Q insists that the mere mention of the word “autism” provokes a negative response by BHOs and CMHCs. “You can almost hear the screeching of the brakes at the other end of the line.” But Q argues, as do many others (including clinicians), that Autism disrupts communication and social skills, resulting in behavioral symptoms that can be treated in the same way that behavioral symptoms associated with mental illnesses can be treated. However, Colorado Medicaid distinguishes between behavioral problems that are a result of Autism (or other developmental disabilities), and identical behavioral problems that are a result of a mental illness.
Q noted one of the most oft-cited disconnects resulting from this artificial distinction (discussed in more detail below): That Applied Behavioral Analysis (ABA) is an autism-specific treatment that has a behavioral health billing code. This means that ABA can only be accessed if the patient has a mental illness diagnosis, despite the fact that Autism (for which ABA is considered the standard of care) is categorized as a medical diagnosis. Q discussed (as did many other providers and advocates in my conversations with them) the need this imposes on parents and providers to rely on creative coding and labeling to navigate the system.
Q reiterated another frequently repeated observation: That it’s hard to imagine someone who isn’t a professional advocate, or otherwise thoroughly versed in the intricacies of the system, navigating the system. Q observed that there are three systems that have to deal with and pay for children’s maladaptive behaviors: Education, Health Care, and Juvenile Justice. Each wants to shift the burden to the others. And since Juvenile Justice is the only one that can’t deny services, too many children in need of behavioral health services end up in the Juvenile Justice system.
Case Study Three.
E (child), who is diagnosed with psychotic disorder, autism, and mood disorder, has long suffered from explosive tantrums, auditory and visual hallucinations (sometimes “advising” him to act violently), anger, obsessive behaviors, volatile mood swings, and other symptoms. E is a teen-age male, who, like C in Case Study One, poses a risk to self and others. At home, E is often aggressive and demanding, damaging property, having difficulty with personal hygiene, and in general lacking independent living skills. R (parent) was particularly concerned for the safety of a much younger sibling also living in the home.
Despite these symptoms, as in the case of C described in Case Study One, the parent and other adults who have had contact with E describe him as “a sweet kid.” They perceive the symptoms of his mental illness to be distinct from his essential character as a human being.
E was placed in a succession of out-of-classroom programs by the school district, from kindergarten onward. He has relied on outpatient therapy and medication nearly all his life. He was hospitalized several times due to his behaviors at home. The BHO refused to pay for his last hospitalization, claiming that it was not due to a covered diagnosis.
R (parent) originally sought day treatment for E, in which E could receive both mental health and educational services, which had previously proven very useful. The BHO denied day treatment for E, insisting that in-home treatment was more appropriate and less costly. E’s doctors were adamant that E needed day treatment, that it was a medical necessity. The BHO insisted that the behavioral issues were due to E’s developmental disability rather than a covered mental illness (despite the ample mental illness diagnoses), and that day treatment “wouldn’t do him any good,” despite the fact that it had done him good in the past, and that his doctors adamantly recommended it for him.
In the course of negotiations on this matter, the BHO tried to place responsibility for E’s mental health care on the school district, insisting that it was a problem for Special Education to deal with. Eventually litigation was threatened, and the BHO made some concessions to avoid it, reversing its decision regarding day treatment, but authorizing it for an insufficient length of time. R continued to struggle with the BHO over the provision of appropriate and necessary mental health services for E.
R agreed to try in-home therapy, but it has not been very successful. Due to the continuing threat to the safety of E himself and others in the household, E’s psychiatrist and his clinician both recommended residential care for E, stating that “out of home placement in a residential setting is strongly indicated . . . [T]his level of care has the potential to improve [E’s] psychiatric status and his functioning. [E] has responded best to a structured, supportive, therapeutic setting.”3 Despite these strong recommendations, the BHO refused residential care, stating that “[E’s] psychotic symptoms would not be expected to benefit from or require residential treatment level of care.”
R appealed the BHO’s decision, and received several independent evaluations confirming the need for residential care for E. In the light of this overwhelming evidence contradicting the BHO’s refusal of services, an Administrative Law Judge recently reversed the BHO’s decision to refuse residential services to E, ordering that the services be provided.
Anecdotal Evidence of Informal Denials (or “Non-Denial Denials”).
Almost all of the parents I interviewed reported similar experiences of receiving “informal denials,” either prior to, or in place of, formal ones (known as a “Notice of Action,” or NOA), which are necessary to initiate a grievance or appeal. In one particularly revealing incident, a CMHC had accidentally sent the parent the evaluating physician’s confirmation that the child had a covered mental health diagnosis and was eligible for services. But the CMHC then informally denied that child services, neglecting to send a letter of denial. Another parent reported that her CMHC refused mental health services to her child with a mental illness, who had suffered a brain injury sometime after receiving his mental illness diagnosis, because “we don’t treat medical conditions here” (implying that since a brain injury is a medical condition, all behavioral problems will be attributed to it, despite the fact that the bipolar diagnosis predated the brain injury). A BHO official confirmed this decision, showing this parent the contract, in which it is stated that the BHO is not responsible for medical problems. No Notice of Action was issued.
One parent spoke of the confusing forms, the inflexibility of in-take policies and procedures, how when laryngitis made it impossible for her to participate in a scheduled telephone call, she was kicked back to the beginning of the entire process of applying for access to services. She was not provided with information about respite care when she inquired into it. This parent, too, stated that she is not able to access services for her child if she mentions that the child has a developmental disability as well as a mental illness, without an NOA ever being issued.
Several parents, most advocates, and even many providers indicated that such informal denials occur with great frequency at various stages in the process, from intake to post-evaluation. Reports include clients being told by in-take personnel that violent behaviors by the child preclude eligibility for Medicaid covered mental health services, that such behaviors are a matter for the police and not for mental health care providers, or that network providers would have to be used but receiving outdated provider lists with disconnected numbers or otherwise inaccessible or non-existent providers. Clients (particularly adoptive parents) have also reported being inappropriately referred to social services for conditions that are Medicaid’s and not social services’ responsibility to address.
Section Four: BHO Formal Denials Data
According to the data provided to me by CBHC and the five BHOs, out of a total of 58,115 child and adolescent clients served (all children and adolescents served through the BHOs, according to Brian Turner of CBHC not just those on Medicaid or those with multiple diagnoses), there were 54 denials based on Co-Occurring Disorders (almost half by one BHO) issued by all five BHOs to no more than 49 individuals (not all BHOs indicated when multiple denials were issued to the same person) over an 18 month period. This data does not suggest a high rate of such formal denials, but three things should be born in mind: 1) We have not been provided with the relevant denominator, which is the total number of multiple-diagnosis Medicaid eligible children served, to determine what portion of those children are denied services due to their co-occurring conditions; 2) most of the personal stories related to me don’t involve the issuance of NOAs (and thus are not included in this data) but do result in denials of services, raising the question of the prevalence of “informal denials;” and 3) this is self-reported data by the BHOs that cannot be verified, and is not subject to any independent oversight.
To underscore these points, one BHO reports only 8 denials for 6 individuals during the 18 month period under consideration, though one of the CMHCs affiliated with it has a widespread and intensely felt reputation among the mental health advocates and providers I talked with for overzealous denials of services, particularly to multiple diagnosis children. (One professional, in no way affiliated with that CMHC, told me that the medical director of that CMHC has explicitly stated that he considers any behavioral problem that occurs in a child with a developmental disability to be by definition a neurological rather than a mental health problem, and thus never the result of a covered diagnosis, despite the protocol developed to ensure that such blanket denials of mental health services to children with developmental disabilities are not public policy.) Conversely, another BHO which includes a program with a stellar reputation for ensuring that multiple diagnosis children receive appropriate services, reports 11 denials of services, and gave by far the most complete and detailed information for each case of all five BHOs.
While the 54 formal denials of services to those children with co-occurring conditions, representing less than one thousandth of the total number of child and adolescent clients served, may not seem like an alarmingly high rate of occurrence, it is nevertheless a heavy burden for the families involved, and may represent a pattern of treatment toward a particular subclass of clients. Furthermore, this data gives us no insight into how many families were informally denied services, by being turned away before any official request for services was recorded.
Section Five: An Analysis of Relevant Issues
There are clearly numerous human, social, fiscal, and economic costs implicated in the failure to address this problem. The human costs borne by the individuals and families directly impacted are enormous, and well-represented by the anecdotal evidence reported above. The social costs include increased prevalence of socially maladaptive behaviors that can at times become violent or criminal in nature. The fiscal costs are typical of those borne by society when we are “penny wise and pound foolish,” failing to invest in proactive policies that reduce far larger and more cumbersome reactive costs. One simple and obvious example is the overreliance on expensive emergency room care for chronic conditions when less expensive and more effective appropriate preventative treatment is recommended. The economic costs include reduced productivity and an increased burden on our juvenile justice and criminal justice systems due to the failure to proactively address this and related problems.
In order to avoid these numerous and onerous costs, we need to meet the challenge of resolving The Co-Occurring Disorder Dilemma. The major interrelated structural problems that need to be addressed and rectified are:
1. The bifurcation of capitated Medicaid for mental health problems, and fee-for-service Medicaid for “medical” problems (which include co-occurring conditions such as developmental disabilities, ASD, TBI, and fetal alcohol syndrome), despite the fact that this distinction often segregates identical behavioral problems requiring identical treatments, distinguished only by the context in which they occur.
2. The distinction made between identical behavioral symptoms according to the presence or absence of diagnostically and clinically independent co-occurring conditions.
3. The need to align covered diagnoses (i.e., diagnoses that are covered under either fee-for-service “medical” Medicaid or capitated “behavioral” Medicaid) with covered treatments in the same silo (i.e., treatments that carry a billing code that falls into either fee-for-service or capitated Medicaid, matching the silo of the covered diagnosis). This is exacerbated by possibly overly-restrictive authorization of providers, even though clinical best practices require a more fluid matching of treatment, diagnosis, and provider according to particular confluences of circumstances.
4. The insufficient cross-training of mental health care providers in issues specific to people suffering from co-occurring conditions (particularly DD and ASD).
5. Insufficient integration of services and coordination of service providers.
6. Insufficient assistance to clients trying to navigate the confusing and convoluted behavioral health care system.
7. Insufficient tracking and oversight of formal denials of services by independent contractors paid a set fee to manage the provision of mental health care services under Medicaid.
8. Non-existent tracking and oversight of the apparently more pervasive informal denials, such as clients potentially eligible for services being told on the phone or at the front desk that they are not.
9. Insufficient training of in-take personnel, leading to an increased frequency in the occurrence of informal denials.
Structural problems 1-5, above, can be categorized as “siloing” problems. “Siloing” refers to a separation and lack of coordination among interrelated services, agencies, and procedures. Siloing is widely understood among those involved in publicly provided human services to be a fundamental structural problem, obstructing the efficient and effective delivery of services. Siloing clearly is a major factor contributing to the difficulties facing families of multiple diagnosis children and adolescents.
The first type of siloing listed above is the administrative lynchpin of the problem. Diagnostically and clinically identical maladaptive behaviors can fall into one of two administratively distinct categories: Fee-for-service “medical” Medicaid, or capitated “behavioral health” Medicaid. The latter include behaviors deemed to be caused by a diagnosed mental health disorder, and thus the responsibility of the BHOs and their provider networks to cover. The former include behaviors that are deemed to be caused by any of various co-occurring conditions (Autism Spectrum Disorder, Developmental Disability, Traumatic Brain Injury, Fetal Alcohol Syndrome), and thus the responsibility of fee-for-service Medicaid to cover.
The second, closely related, example of siloing implicated in the Co-Occurring Disorder Dilemma is the segregation of exhibited behavioral problems into those associated with a mental illness, and those associated with some other co-occurring condition. According to Dr. Judy Reaven, a child psychologist with JFK Partners at the University of Colorado School of Medicine, there is no diagnostic or clinical justification for this distinction. There is general agreement with this view among other clinicians I spoke with, such as Cory Robinson, Director of JFK Partners, and Dr. Marianne Wamboldt, Chair of the Department of Psychiatry and Behavioral Sciences at Children’s Hospital. All three agree that this is the prevailing view among clinicians.
Dr. Reaven emphasizes that there is no basis for distinguishing behavioral problems manifested by a child (or adult) with a developmental disability and behavioral problems that are symptomatic of a mental illness. Neither in terms of what we know about underlying causes, nor in terms of the efficacy of standard treatments, does such a distinction have any justification. Since there appears to be no medical basis for making such a distinction, it is an administrative artifact which serves as an obstacle to the implementation of clinical best practices, and facilitates the denial of mental health services to those who both need them and, by law, are entitled to them.
In Dr. Reaven’s words:
Related to the artificial distinction between “behavior” that is symptomatic of DD vs. a mental health condition, is that clinicians are asked to independently treat “mental illness,” and “autism or other DD” knowing full well that diagnostic complexity exists in most of the patients we see. It is nearly impossible to identify the specific symptoms that are only ASD vs. symptoms that are only mental illness. Finally – best practice would suggest that clinicians consider the whole child, as knowledge of the whole child must inform the specific treatment and modifications necessary for enhanced efficacy of the intervention. Not allowing clinicians to even acknowledge the complexity of patient’s presentation in many cases can lead to a superficiality of treatment.
Related to this is a phenomenon known as “diagnostic overshadowing” (coined by Steven Reiss in 1983), a tendency to disregard the diagnostic indicators if behaviors can be attributed to a developmental disability instead of to the mental illness diagnosis consistent with the behaviors, even though the presence or absence of the developmental disability is generally not diagnostically relevant. Again, in Dr. Reaven’s words:
Diagnostic overshadowing refers to the tendency to attribute behavioral challenges and mental health symptoms in an individual with DD or ASD, solely to the developmental disability or ASD, rather than assign an additional mental health diagnosis, even if the symptom presentation are all consistent with such a diagnosis; in other words, mental health symptoms are “overshadowed” by the DD/ASD and as a result are not appropriately identified or treated.
While co-occurring conditions can be clinically relevant, just as any number of other contextual factors can be, their presence does not generally imply that the use of standard mental health treatments and therapies will be ineffective, only that such treatments need to be adapted appropriately to the needs of the individual child, as is always the case. So, for instance, if a child has a developmental disability that affects his or her ability to communicate verbally, this is a factor that must be taken into account, not a factor which renders irrelevant the child’s mental health treatment needs.
According to the 2011 Ombudsman’s Report, BHOs do (and are contractually authorized, perhaps required, to do) precisely what Dr. Reaven described above as impossible and irrelevant to do: differentiate between similar behaviors as in some cases an artifact of a developmental disability and in other cases an artifact of a mental illness. According to the report, regardless of the diagnoses that exist, there is “a reluctance on the part of plans to approve treatment services for behaviors that may be caused by a medical diagnosis (autism or traumatic brain injury) which are then exacerbated by mental health conditions, or vice versa” (emphasis added). The key phrase above is “may be,” because, while the BHOs are contractually empowered to make such distinctions, they are rarely diagnostically or clinically justifiable.
Marceil Case of the Colorado Department of Health Care Policy and Financing (HCPF), the state agency which oversees Colorado Medicaid, stated at one point, in an interview with me, that if the BHOs determine that there is a mental illness diagnosis, then the BHOs are responsible for covering behaviors that are associated with that diagnosis, regardless of whether the client has a co-occurring developmental disability. The ambiguity of this statement sheds some hazy light on the nature of the problem, because the determination to provide or deny services hinges on whether the BHOs determine that the behavior meets the higher threshold of being caused by the diagnosis, rather than the more clinically meaningful threshold of being consistent with the diagnosis.
In fact, BHOs are authorized (perhaps required) to deny services for behaviors “associated with” a covered mental health diagnosis, if the BHO asserts that the behaviors are the result of a co-occurring condition rather than of the covered mental illness. Given that making such determinations reduces costs incurred by the BHOs, that such determinations can be and are at times made in opposition to clinical recommendations, and that such determinations are not automatically reviewed, it is economically axiomatic that such determinations are likely to be made excessively.
But even were the clinically more relevant criterion relied on, that any behavior requiring treatment that is “consistent with a covered mental health diagnosis” be covered, it still would leave open a large loophole through which services can be denied: It is left to the BHO’s discretion to determine whether such a mental health diagnosis actually pertains, a determination not bound even by what their own CMHCs or independent mental health providers may say. Therefore, the BHOs are free to claim that a behavioral problem exhibited by a child with a developmental disability is the result of the developmental disability rather than of a mental illness, even if that child has been clinically diagnosed with a mental illness, and even if they were obligated to provide services for anyone they deem to have a covered diagnosis (which is not currently the case). In practice, the BHO has complete discretionary power to determine whether the child has or does not have a covered mental health diagnosis. And, again, such determinations are not subject to automatic review.
In other words, the BHOs have complete discretionary authority to determine, independently of clinical recommendations, both whether a client exhibiting behaviors consistent with a covered mental health diagnosis actually has that diagnosis, and whether, if so, the exhibited behaviors are the result of that diagnosis. (The decisions can be appealed by the client, but the nature of the problem at hand is, in part, that there are so many obstacles strewn in the paths of clients. There is such a maze of bureaucratic hoops to jump through, that already overburdened parents and guardians seeking behavioral health services for their multiple-diagnosis children find themselves forced to become assertive self-advocates. As a result, they must either dedicate considerable time and effort that they can ill-afford, or fail to obtain services to which they are entitled.)
The third type of siloing listed above requires that only therapies that carry a billing code associated with one or the other of the two administrative silos (capitated or fee-for-service) are administered only for diagnoses that are covered under that same administrative silo. In other words, a therapy coded as a behavioral health treatment cannot be used for a diagnosis whose billing code is fee-for-service, even if that therapy is the standard of care for that diagnosis. This administrative requirement obstructs rather than facilitates clinical best practices: Appropriate and covered therapies should be provided for appropriate and covered diagnoses, by any qualified and competent service provider.
The consequences of failing to allow any covered therapy to be provided by any authorized and qualified behavioral health provider for any covered diagnosis is to effectively deny covered services for covered diagnoses to eligible recipients; to reduce the quality of care to many of those who do receive services; and to force frustrated providers to work around these arbitrary obstacles by making a mockery of the labels that impose them in the first place.
Brian Tallant, the program director at Intercept Center (a joint program between Aurora Mental Health Center and Aurora Public Schools discussed below), offers the following example of this problem:
Best practices for the treatment of Autism is a combination of Applied Behavioral Analysis (ABA), speech/language therapy and occupational therapy. ABA is considered a behavioral health service, and typically has a behavioral health CPT (Current Procedural Terminology) code that corresponds to that service. Speech/language therapy, as well as occupational therapy, are medical services and have corresponding medical CPT codes. Capitated (Behavioral Health) Medicaid has a list of covered psychiatric diagnoses, but excludes Autism as a neurological or medical condition, and therefore ABA interventions are not authorized based on the diagnosis of Autism. If a clinician provides ABA services under the diagnosis of Autism, and tries to bill medical fee-for-service Medicaid for ABA services, using behavioral health CPT codes, it is often rejected as being a “behavioral health” service, which should be covered by Capitated Medicaid. So you see how a child with Autism is caught between a system that excludes their behavioral treatment either by diagnosis (Capitated Medicaid), or by service code (medical fee-for-service Medicaid).
Brian Tallant describes how the provider is also caught up in the siloing of particular treatments for a particular diagnosis:
[T]he problem mostly rests with Applied Behavior Analysis (ABA), or other “behavioral” services, that are provided by a professional that has more of a behavioral health training and/or certification. These professionals can provide services that are best described by behavioral health service codes (ICD-9 codes), when they are authorized and approved for treatment of a covered diagnosis under capitated Medicaid. If a person has a medical diagnosis (excluded mental health diagnosis), such as autism or TBI, the behavioral therapist does not have medical ICD-9 codes that allow for billing under fee-for-service Medicaid. Behavioral services codes are rejected by fee-for-service Medicaid as being “behavioral health” services, even though they are qualified to provide those services, and they are treating a medical condition.
While this may be little more than a restatement of the problem of having to align covered diagnoses and covered treatments under a single silo, it draws attention to the fact that a provider fully qualified to provide the treatment that represents best practices for a given diagnosis may be prohibited from providing that treatment, simply as a result of how the treatment is coded.
The fourth and fifth types of siloing listed above involve the siloing of expertise, both by a lack of cross-training of service providers, and a lack of coordination among service providers. Due to a lack of cross-training, clinical assessments are made by service providers who may not understand the relationships between, for instance, developmental disabilities and mental illnesses, and thus make diagnostic and clinical judgments that are only partially informed. Due to the lack of coordination among service providers, clients seeking services in one silo may not be directed to services appropriate for them offered in another. This siloing of expertise exacerbates the interacting dysfunction of the first three administrative forms of siloing by reproducing and reinforcing it at the level of service provision.
The final four structural problems listed above are not siloing problems, but are rather problems in assistance to clients and oversight of managed care providers. They interact with the five siloing problems by leaving clients to fend for themselves in a system posing numerous obstacles to their ability to access appropriate services.
Many parents of multiple diagnosis children who are also knowledgeable advocates for the interests of multiple diagnosis children note that no one who is not a trained advocate could possibly hope to navigate this convoluted and obstruction-strewn system effectively. The anecdotal evidence is rife with stories of parents being misinformed, misdirected, and given a general run-around, while dealing with the other onerous burdens of raising developmentally disabled and mentally ill children. Clearly, this nightmarish maze that such parents must try to negotiate, against obstacles both intentional and unintentional, is a major part of the problem with how this system functions…, or fails to.
This bureaucratic labyrinth, which serves interests other than those of the clients who need to access the system, is left largely unchallenged due to a lack of administrative resolve and oversight. No state agency or advocacy organization is tracking formal denials of mental health services other than the independent (two nonprofit and three for-profit) contractors that have a financial incentive to deny them. No state agency or advocacy organization is extracting and analyzing information about the reasons given for denials in cases that are aggrieved or appealed. No state agency or advocacy organization is attempting to systematically track or assess the apparently far larger problem of informal denials, in which applicants are obstructed from accessing services to which they are entitled in ways that do not result in a formal Notice of Action (NOA). The first step to remedying the Co-Occurring Disorder Dilemma is to rectify this glaring lack of data collection and administrative oversight, and the enabling lack of sustained, focused advocacy insisting on such data collection and oversight.
Clearly, the imposition of new administrative burdens is not to be taken lightly. But the glaring deficiency in this case suggests that perhaps the current distribution of administrative burdens is not optimally targeted.
Section Six: An Example of a Program That Works Well
Intercept Center
Intercept Center is a joint program of Aurora Mental Health Center and Aurora Public schools, established in 1995, to accommodate the educational and behavioral health needs of Medicaid-eligible children from ages 5 to 21 with both a covered mental health diagnosis and a developmental disability. Aurora Public Schools provides the building, special education teachers, paraprofessionals, instructional materials, and itinerant special education staff and services, while Aurora Mental Health Center provides the mental health treatment services and personnel. Aurora Mental Health Center and Aurora Public Schools are currently putting together a Memorandum of Understanding to more fully formalize this joint venture.
Intercept Center operates as both a school and a day treatment center, with students receiving both their educational and behavioral health treatment needs in one location and under the auspices of one program. Intercept Center also functions as an intensive services outpatient clinic for multiply diagnosed children in the Aurora area. The relative success of Intercept Center in reducing or eliminating the gap in services encountered by many multiple diagnosis children on Medicaid is due, in large part, to the training of the mental health service providers there, and the assertive coordination with other facilities and programs to accommodate needs that fall beyond the parameters of the services that Intercept Center provides.
The success of such a program requires the willingness of the overarching Behavioral Health Organization (in this case, BHI), to permit a more rather than less inclusive determination of eligibility for services, and the stewardship of a program director (in this case, Brian Tallant) committed to ensuring that applicants receive any and all services to which they are entitled, whether under the auspices of this program, or through another service provider more appropriate to that particular child’s needs. Unfortunately, under our current overarching system, the satisfaction of these two necessary conditions is the exception rather than the rule.
While Intercept Center does not currently bill fee-for-service Medicaid to provide (“medical”) services that are not covered under capitation (“mental health services”), it does coordinate with providers who do. Aurora Mental Health Center is contemplating expanding the Intercept Center program to provide behavioral services that are covered under fee-for-service Medicaid, as well as the behavioral services that are covered under capitated Medicaid.
Intercept Center does not provide residential services, but has a close relationship with Smith Agency, which is a child placement agency for foster care, and the provider of Serenity Group Homes and Serenity Learning Center. Intercept identifies children who need residential treatment, informs parents of the procedures to go through and of the various options available to them. In one case, Intercept assisted foster parents in expanding their business into a group home, which they wouldn’t have been able to do without Intercept’s support and guidance. Intercept Center providers also go into Residential Child Care Facilities (RCCFs), which serve children with developmental disabilities, to provide certain mental health services on-site (particularly, capitated Medicaid-covered individual and group therapies), but children in RCCFs must come to Intercept Center for medication to be administered.
Intercept Center is evidence of the fact that it is possible to design and implement a relatively well-functioning model under the auspices of Colorado’s current Mental Health Medicaid system, but also, in its exceptionalness, of the fact that such models are not the inevitable by-product of that system. To the extent that we continue to operate within current parameters, one immediate goal is to ensure that the Intercept Center model is replicated as widely as possible. To the extent that we change those parameters, one intermediate goal is to ensure that the lessons of Intercept Center inform systemic and mandatory changes.
Section Seven: Possible Solutions and Recommendations
An Overview of Policy Goals
The principal recommendation of this report is that the relevant governmental agencies systematically research and remedy The Co-Occurring Disorder Dilemma, with persistent resolve and unflagging determination. Since this has not yet happened, and there is no evidence of it spontaneously occurring, the secondary recommendation is that all relevant advocacy groups place sustained, informed pressure on those governmental agencies and office holders to do so. The State of Colorado needs to commission a comprehensive study, incorporating data that either currently does not exist or cannot be accessed, and, based on that study, design and implement an affirmative plan to rectify the obstacles to access to mental health services faced by children and adolescents with co-occurring conditions.
The state has a number of options for addressing and rectifying the major interrelated structural problems listed in section five, above. We need to design and implement a set of policies which:
1. Eliminates the effect of bifurcation of Medicaid into capitated and fee-for-service enclaves, either by (ideally) eliminating the bifurcation itself or (more practically) perforating the wall between them sufficiently that it ceases to obstruct the diagnostically and clinically appropriate and necessary provision of services.
2. Eliminates the effect of administrative (diagnostically and clinically unjustifiable) segregation of identical behavioral problems according to whether they are administratively deemed to be the result of a mental health diagnosis or some co-occurring condition.
3. Eliminates the need to align providers, diagnoses, and treatments under one or the other of the two Medicaid silos described in numbers 1 and 2, above. This primarily involves eliminating the need to provide only behavioral therapies and treatments with a billing code that corresponds to the silo (either fee-for-service or capitated) that the behaviorally related diagnosis is covered under. A more flexible system is needed to ensure that any covered treatment for any covered diagnosis can be provided by any competent and qualified behavioral health service provider.
4. Ensures that behavioral health providers are appropriately cross-trained to know how to effectively diagnose and treat co-occurring developmental disabilities and mental illnesses.
5. Ensures the integration and coordination of services and service providers.
6. Ensures the shifting of the burden for navigating the complex and confusing behavioral health care system away from overwhelmed clients often poorly equipped to take on such a challenge, and onto designated and adequately trained personnel within the system itself.
7. Ensures comprehensive tracking and analysis of denials of services by responsible governmental agencies, and the exercise of adequate oversight of the BHOs contracted to manage the provision of covered services to those who are entitled to them. (The bureaucratic burden of doing so must be taken into account, and a careful cost-benefit analysis pursued, but it is clear that we currently have a sub-optimal level of such tracking and analysis in place, essentially “leaving the fox in charge of the henhouse.”)
8. Ensures a dedicated investigation and rectification of informal procedures by which services may be denied without any formal request for services ever being recorded, and thus no formal denial ever being issued.
9. Ensures that in-take personnel and other gate-keepers are adequately trained to record and follow up on all requests for services, to turn no one away on the basis of any peremptory assumption that clients seeking services are not entitled to services.
The structural factors and associated policy goals listed above fall into three categories: Gateway Problems (6-9), Service Provision Problems (4-5), and Underlying Structural Problems (1-3). The Gateway Problems are problems at the point of interface between clients and the mental health care system. They involve insufficient oversight of the formal and informal ways in which clients are refused services (7 and 8, respectively), and insufficient guidance and inaccurate information provided to clients seeking services (6 and 9, respectively). The Service Provision Problems are problems that affect access to services by dispersing rather than consolidating service provider expertise. They involve insufficient expertise regarding multiple diagnosis issues within individual service providers (4), and insufficient coordination of expertise among service providers (5). The Underlying Structural Problems are problems embedded in the administrative structure of Colorado Medicaid. They involve, collectively, an incongruence between the administrative structure for the delivery of mental health services, and the clinical reality of the delivery of mental health services.
Specific strategies for addressing the Co-Occurring Disorder Dilemma involve addressing specific combinations of the above policy goals for specific purposes. For instance, as Intercept Center’s success illustrates, by addressing the Service Provision Problems and one Gateway Problem -numbers 4, 5, and 9- local programs can dramatically reduce the Co-Occurring Disorder Dilemma on their own initiative (and with the support of their BHO). By concentrating and coordinating expertise in both mental illness and developmental disabilities, and ensuring that there is an open gateway to that consolidated expertise, a local program can distinguish itself even in the context of the other six unresolved structural problems.
Numbers 4, 5, and 9 can be addressed proactively, by any BHO or CMHC that chooses to take the initiative. Thus, significant local improvement in the provision of services to multiply diagnosed children can be accomplished even in the absence of statewide public policy changes. However, a sustainable and reliable statewide paradigm shift will almost certainly require overarching public policy refinements. And even such relatively successful local programs as Intercept are limited in the degree to which they can effectively address the Co-Occurring Disorder Dilemma by a lack of facilitating statewide policies.
The remaining Gateway Problems and related policy goals, 6-8, suggest a second strategic avenue comprised of direct advocacy for immediate and easily implemented administrative reforms. These do not require any major structural changes, simply superficial changes in policy that, for instance, provide clients seeking services with personnel competent to guide and inform them, and implement more diligent administrative oversight of the mental health managed care system.
Finally, the far-reaching statewide administrative structural changes conducive to eliminating or reducing the Co-Occurring Disorder Dilemma are summarized in numbers 1, 2, and 3, above. These would require significant legislative and administrative action, and are thus higher hurdles to clear. Progress on Underlying Structural Problems neither requires nor is a requirement of progress on either Gateway or Service Provision Problems. Long-term structural strategic goals and short-term immediately ameliorative strategic goals can be pursued independently and simultaneously.
A recommended comprehensive strategy for those who choose to act on this report, therefore, is to seek immediate widespread, either centrally directed or CMHC by CMHC, implementation of 4, 5, and 9, while simultaneously working toward both the superficial administrative policy changes suggested in numbers 6, 7, and 8, and the eventual implementation of long-term policy goals 1, 2, and 3.
A Survey of Specific Solutions
This section briefly examines examples of three different kinds of approaches to addressing The Co-Occurring Disorder Dilemma: 1) a broadly applicable and assertive social institutional approach (Medical-Legal Partnership), 2) a managed care-level administrative approach (Expanded BHO Contract), and 3) a flexible and accommodating provider-level administrative approach (The Medical Home Model). These three approaches are not mutually exclusive; they can be combined in part or in whole to form a comprehensive strategy for addressing The Co-Occurring Disorder Dilemma.
Medical-Legal Partnership: Medical-Legal Partnerships (MLPs) involve integrating lawyers into the health care team available to clients, to address the non-medical factors affecting their health. As The National Center for Medical-Legal Partnership (NCMLP) puts it:
Medical-legal partnership (MLP) is a new patient care model that aims to improve the health and well-being of vulnerable individuals, children and families by integrating legal assistance into the medical setting. MLPs address social determinants of health and seek to eliminate barriers to healthcare in order to help vulnerable populations meet their basic needs and stay healthy.4
One form of MLP is the inclusion of lawyers on a health care provider team to address exacerbating conditions that health care providers are neither qualified nor empowered to address, such as mold-infested housing aggravating the condition of an asthmatic child, or lack of food and heat creating health risks that cannot be resolved through medical treatments alone. In a sense, this is another reduction of “siloing,” such that the various kinds of circumstances that combine to create or exacerbate medical problems can be addressed in tandem with the medical treatment itself.
More generally, a Medical-Legal Partnership is the combination of advocacy and medical treatment, so that patients’ rights are protected in service to the provision of adequate health care that is not divorced from the broader social institutional context in which it occurs. As the above quote from the NCMLP website illustrates, such legal advocacy integrated into the “medical setting” could serve a vital role in placing sustained pressure on Colorado Medicaid’s administrative apparatus to address and resolve the structural defects that result in The Co-Occurring Disorder Dilemma. More broadly, the establishment of Medical-Legal Partnerships throughout Colorado’s health care system would provide institutionally integrated patient advocacy to address all such problems as they arise.
In the present context, a Medical-Legal Partnership would involve an alliance of behavioral health care providers and legal advocates working together to ensure that their clients receive the full range of behavioral health care services to which they are legally entitled, and to ensure that the services received are accessible, coordinated, and appropriate.
Expanded BHO Contract: One possible solution to the difficulties faced by families of multiple diagnosis children, favored by the Colorado Behavioral Healthcare Council (CBHC, the umbrella organization for the BHOs), would be to expand the state’s contract with the BHOs to include in their mandate responsibility and compensation for providing all covered services for all covered behaviorally related diagnoses, whether currently categorized as mental illness or in some other way (such as a by-product of a developmental disability). Another, similar solution would involve authorizing and equipping BHOs and CMHCs to provide all behavioral services, some covered by capitated Medicaid, and some charged to fee-for-service Medicaid, according to their billing codes. These solutions would address some of the factors contributing to the current systemic deficiency, but would leave many of the other contributing factors intact. As such, they are, at best, partial solutions.
Some advocates are concerned that these solutions would merely perpetuate the problem in a new guise, since the BHOs, intended as cost reducing intermediaries, are incentivized to deny services whenever possible. This may be a legitimate concern, but, when coupled with the Medical-Legal Partnership approach described above, the added vigilance thus provided might help to mitigate and counterbalance any overzealousness to deny services on the BHOs’ and CMHCs’ part. This combination might be a robust way to institutionalize, as a permanent feature of the Medicaid behavioral health landscape, a vehicle for negotiating the inherent tension between efficiency (i.e., cost-cutting) and protection of patients’ rights.
Medical Home Model: The Medical Home Model (sometimes called “patient-centered medical home,” or PCMH) involves a centrally coordinated, continuous and comprehensive system of care led by a primary care physician. Intercept Center (described above) incorporates some elements of the Medical Home Model, in which the program director coordinates with other service providers to deliver coordinated and comprehensive care (and educational services) to children in the program. As discussed above, using Intercept Center as an example, the Medical Home Model is most adept at addressing issues 4, 5, and 9 (cross-training of service providers, coordination and integration of services, and better assistance to clients in navigating the system). The Medical Home Model is often considered the best way to keep children with mental illnesses, developmental disabilities, and Autism Spectrum Disorder in the least restrictive environment, and provided with the most comprehensive and appropriate treatment plan.
In the context of reducing the effects of siloing in Colorado Medicaid’s delivery of behavioral health services, the Medical Home is a potentially essential partner to higher level solutions. If, for example, the BHOs’ contract were to be broadened to include management of care for all behaviorally related conditions, the Medical Home would be the ideal vehicle for coordinating and integrating that care. Thus, in one possible integration of these three approaches, the Medical-Legal Partnership could hold the BHOs accountable, while the Medical Home could implement their comprehensive mandate on the ground.
Conclusion
A combination of inherent financial incentives, excessive discretionary power by independent contractors, inadequate oversight, inadequately trained personnel, and inadequate availability of mandatory services helps to produce the gap in services experienced by children and adolescents with multiple mental health and developmental disability (or other “medical”) diagnoses. An administrative structure comprised of siloing in multiple, interacting ways (in terms of diagnoses, treatments, providers, and billing) obstructs rather than facilitates the coordination of services. And a lack of resolve among responsible agencies has left this problem largely unaddressed.
Previous attempts to close this and related gaps have proven insufficient. Protocols for clients with co-occurring DD and MI diagnoses, and co-occurring TBI and MI diagnoses, have done little to solve the problem. The Child Mental Health Treatment Act (CMHTA, or “HB 1116”), designed to provide access to residential treatment services without recourse to Social Services (which generally requires a Dependency and Neglect action, exposing parents to the risk of losing custody of their children in order to access vital services), has too often simply been disregarded or misunderstood. General awareness of the Co-Occurring Disorder Dilemma is widespread among advocates, affected clients, and individual service providers, but sustained pressure to resolve it has not yet been applied.
This difficulty in accessing necessary services, sometimes essential to the safety of the affected child and others in the child’s household, imposes an onerous burden on families already overburdened with the challenges of caring for children with multiple mental health and developmental problems. Solutions exist and can be implemented, ranging from the local and partial to the systemic and far-reaching. It is incumbent on all stakeholders to do their part to ensure that these solutions are implemented.
Methodology
The research for this report consists primarily of meetings and conversations with 1) parents who have had difficulties accessing mental health services for their multiple diagnosis children; 2) professional advocates for those with mental illnesses and developmental disabilities (frequently also parents of mentally ill or developmentally disabled children); 3) the executive director of an advocacy organization for adoptive families (adoptive families being disproportionately impacted by this problem); 4) Mental Health program directors and service providers; and 5) governmental agency officials and contractors.
Among the governmental agency officials, nonprofit executive directors, advocates and service providers I interviewed, met with, or corresponded with in the course of researching this issue are Marceil Case (HCPF Mental Health Specialist), George DelGrosso (Executive Director of CMHC), Brian Turner (CMHC), Janine Vincent (Ombudsman for Colorado Medicaid Managed Care), Julie Reiskin (Executive Director of Colorado Cross-Disabilities Coalition), Mary Ann Harvey (Executive Director of The Legal Center), Pat Doyle (Rights Advocate at The Legal Center), Deborah Cave (Executive Director of Colorado Coalition of Adoptive Families), KimNichelle Rivera (Outreach/Research Coordinator for Empower Colorado), Judy Reaven (Clinical Psychologist and Director of the Autism and Developmental Disabilities Clinic at JFK Partners, an interdepartmental program of Pediatrics and Psychiatry at University of Colorado School of Medicine), Cordelia Robinson (Director of JFK Partners), Betty Lehman (then Executive Director, Autism Society of Colorado), Marianne Wamboldt (Chair of the Department of Psychiatry and Behavioral Sciences at Children’s Hospital), Brian Tallant (Program Director, Intercept Center, Aurora Mental Health Center), and Sarah McNamee (Early Intervention Service Provider, LCSW).
Among the documents I reviewed while preparing this report are the BHO Contract with the State of Colorado; the Ombudsman’s reports for 2009-2011; the written criteria for BHOs to follow in the treatment of co-occurring mental health diagnoses and traumatic brain injuries; the written criteria for BHOs to follow in the treatment of co-occurring mental health diagnoses and developmental disabilities; a 2009 Primer on the mental health safety net published by the Colorado Health Institute; a 2011 updated report by The Mental Health Funders Collaborative on “The Status of Mental Health Care in Colorado;” a 2004 Urban Institute report on “Access to Children’s Mental Health Services under Medicaid and SCHIP;” a 2008 Department of Health and Human Services Inspector General “Review of Colorado Medicaid Mental Health Capitation and Managed Care Program;” a 2009 DBH and WICHE Mental Health Program “Population in Need” study; a 2008 report commissioned by HCPF on “Colorado’s Medicaid Mental Health Services Program: Issues & Future Direction;” “The Maze,” a 2009 report by Colorado Covering Kids and Families on barriers to access to Medicaid and CHP+ faced by eligible children and families, with a recommendation for streamlined access; some working papers on the clinical issues involved; and various provider and advocacy group newsletters.
Requests for both qualitative and quantitative data regarding the Co-Occurring Disorder Dilemma were made to the Colorado Department of Health Care Policy and Financing (HCPF, the single agency which oversees the Colorado Medicaid program), the Colorado Ombudsman for Medicaid Managed Care, various advocacy groups, and the five Behavioral Health Organizations.
With the exception of the five Behavioral Health Organizations (BHOs) themselves, no one was able to provide any hard data on the prevalence of The Co-Occurring Disorder Dilemma. The various advocacy groups contacted were unable to provide any relevant data other than the shared impression that The Co-Occurring Disorder Dilemma is a pervasive problem. HCPF, in response to a CORA request, provided raw grievance and appeals reports which contained no information relevant to the issue at hand. The Ombudsman did not follow up on an offer to send me relevant data.
With the assistance of George DelGrosso and Brian Turner of the Colorado Behavioral Healthcare Council (CBHC), four of the five BHOs contracted by the state as managed care providers for Colorado Medicaid supplied me with data summarizing the reasons for all of their formal denials, resulting in a Notice of Action (NOA), over the last fiscal year and the first half of the current fiscal year, to child and adolescent Medicaid clients with multiple diagnoses. (Access Behavioral Care, the fifth, provided only the raw number of denials -25- for the 18 month period reported on, and no other information. I was assured that this was due to technical difficulties and not a desire to withhold the information. The CEO of ABC, Rob Bremer, conveyed his willingness, through Brian Turner of CBHC, to work with me one-on-one to fill in that information if I so desired.)
1 For the remainder of the paper, “child” and “children” includes infants through adolescents, until age 21.
2 For the BHO contract and exhibits, see http://www.colorado.gov/cs/Satellite?c=Page&childpagename=HCPF%2FHCPFLayout&cid=1251568046976&pagename=HCPFWrapper.
3 Quotes are taken from the ALJ decision reversing the BHO’s denial of residential services.
4 http://www.medical-legalpartnership.org/
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
As part of A Proposal: The Politics of Kindness, I discussed the importance of organizing and acting in our communities, in non-partisan ways for non-political immediate purposes, in service to the ultimate social and political goal of deepening and broadening the shared commitment to reason and goodwill, in our private lives, in our communities, and in our public policies. I believe that doing so should become a social movement, akin to the Civil Rights Movement, but rather than dedicated to a single issue or set of issues, dedicated instead to a comprehensive attitude that implicates all social issues.
Clearly, the time is ripe for such a movement. Just as the Civil Rights Movement was blessed with a ready-made organizational infrastructure (the southern black church network), so too are all reasonable people of goodwill today blessed with an even more powerful and extensive organizational infrastructure: The Internet and Social Media. I’ve already written about the implications of this technological and social paradigm shift, the possibilities and potentials of which we have just barely begun to explore (se, e.g., A Major Historical Threshold or A Tragically Missed Opportunity?, Wikinomics: The Genius of the Many Unleashed, Tuesday Briefs: The Anti-Empathy Movement & “Crowdfunding”, Counterterrorism: A Model of Centralized Decentralization).
A Tea Partier told me on a Facebook thread recently, “just remember who’s better armed.” When it comes to the more powerful weapons of Social Media, it may be the progressives who are better armed. In any case, the implication of these particular arms is that they accelerate the sifting out of rational from irrational arguments, the lathe of public discourse and debate, which favors reason and goodwill in the long run. Certainly, when it comes to Reason and Goodwill, progressives are better armed, and will inevitably prevail. It is our job to expedite that eventuality, reducing the short-term detours into irrationality and belligerence constantly elongating that path.
The best way to do so is to change the game, the frame and the narrative. Right now, America is stuck in a tug-o-war between progressives and conservatives, both broadly perceived by the vast silent middle to be two opposing extreme camps (with perhaps slightly greater affinity for the conservative than progressive pole). But those same occupants of the vast silent majority would not perceive a movement of community volunteerism and community solidarity building to be either extreme or unattractive. And they would not find it offensive if such a movement included in its “mission” improving the civility and reasonableness of public discourse. But what is the progressive movement if not the commitment to mobilize reason and goodwill, and apply them to our public policies?
The most effective thing progressives could now do is to mobilize a network of Community Action Groups (CAGs) into a nationwide Community Action Network (CAN), dedicated to this component of the proposal linked to above. The only challenge is to create an emerging awareness of the power of such an effort, of the degree to which it can become a game changer if enough progressives were to commit themselves to it. Every local progressive group now in existence, every state house and senate district democratic party organization, every OFA chapter, every MoveOn chapter, every other local group with even moderately liberal leanings, can and should organize into a Community Action Group that seeks to do good works in their own communities, and to foster civil discourse based on no ideology other than a commitment to reason and mutual goodwill.
I ask everyone who reads this to please help me to promote this idea, because the way to become a nation of reasonable people of goodwill is for all who are committed to that end to strive to be reasonable people of goodwill in their own lives, and in their own communities, and to allow that to be a model to others, and to coalesce into a national level commitment. The reason why progressive advocacy is so much less effective than one might think it would be is because progressive advocates are so much less effective, permitting the frames and narratives of the far-right to take root and define the debate. Removing that power from them, and owning it ourselves, is not a function of better sloganeering, but rather of more compelling demonstration; we can and should, we must, demonstrate what it is we are advocating for, if we want our advocacy to become a truly powerful and transformative force in our national history.
Profound lessons come from unexpected quarters. The military, throughout history, has always been a paradoxical social institution, the nexus of the most profound social solidarity but the vehicle of our most violent conflicts; the organization of our basest nature, but the cultivator of our noblest attributes; the realm of brutal action, but the narrative of transcendental philosophies (especially in Eastern philosophies and religions). Therefore, it is appropriate that the most poignant piece of writing I’ve encountered in recent times was an op-ed in today’s Denver Post, describing the ordeal of informing a fallen soldier’s family of the loss of their loved one (http://www.denverpost.com/opinion/ci_16653516).
While the author, Captain Michael Odgers, subtly imports some of the ideological glorification of war that sacrifice facilitates, it is only on the margins of his beautifully written and deeply felt piece. The thrust of the narrative is one of compassion, of feeling the pain of others and taking it on as your own, of knowing that their suffering is our shared burden. I’ve written often that this should form the cornerstone of our national ideology (see, e.g., Our Brothers’ and Sisters’ Keepers). How ironic that the most eloquent expression of the argument should come from the institution that is arguably most biased against it in other spheres of life.
Is the parent’s, the spouse”s, the child’s pain at the loss of their son or daughter, their husband or wife, their mother or father, any less when it occurs in other contexts? Is the compassion that Captain Odgers describes any less appropriate, any less essential, any less necessary to the definition of what it means to be a society?
Not all deaths, even in service to country, occur on the battlefield. Not only do police officers and fire fighters and other rescue workers die in the line of duty, but so do social workers, construction workers, miners, and others making their various contributions to our collective welfare.
But does, or should, our compassion require a down-payment? Must those who have suffered a loss be able to invoke some special claim before they merit our organized and institutionalized moral (and perhaps material) support? Leaving aside the fiscal issues of what we can and can’t afford for the moment, would it be so bad to be a society that cares so much for each and every member that we mobilize such instruments of compassion as Captain Odgers and Chaplain Andy whenever they experience such a loss, or whenver they experience such a need?
I do not deny that we live in a world of limited resources, and that all of our social policies have to be subjected to the cold reality of thorough cost-benefit analyses. But when we engage in those analyses, doesn’t it behoove us to include on the “benefits” side of the ledger the value of institutionalizing assistance for one another when we are in need? We can argue the subtleties within that context, the concerns about “perverse incentives” for instance, but there should be no doubt that what Captain Odgers and Chaplain Andy represent, the institutionalized but absolutely sincere compassion expressed on behalf of a larger society, is a good thing, and it would be just as good a thing in the broader context of a nation (or world) of mutually interdependent and caring human beings, expressing as much goodwill for one another as we possibly can, and making that a cornerstone of who and what we are.
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
I have no idea what motivated the Australian sisters, one of whom died and one of whom survived after a suicide pact at a firing range where they rented the weapons they used on themselves (http://www.denverpost.com/news/ci_16649332). But it is something more than just a bizarre story that grabs our attention, or a private human tragedy made public due to a combination of the circumstances and our own fascination. It is one of the more dramatic expressions of something that is very widespread, and very significant: Human desperation. And of the general challenges we face as a society, the general good we can do together, mitigating human desperation should rank high on the list.
As one commenter on the message board following the Denver Post article said, mental health problems are far more prevalent than most people realize, and the need for better mental health hygiene is nearly universal. All of our social problems are interrelated, usually incubating in troubled childhoods with issues of school truancy or academic failure, child abuse, substance abuse, juvenile delinquency, poverty, and/or mental health issues mixed together in various combinations, reinforcing one another, growing over time.
There are many on the Right who decry “the nanny state,” but we are not enough of a nanny state when it comes to those who most need nannies. We do not invest enough in our children’s welfare –all of our children’s welfare– though the benefits to all of us, let alone those whose lives are essentially saved by being proactive with early interventions, are well worth the investment, and end up saving us not only the suffering inflicted by troubled others, but also the material costs.
The mantra on the Right is that that’s the responsibility of parents. There was a time, just over a century ago, when “child abuse” and domestic violence in general had not yet been defined into existence, because those issues were the family’s business and no one else’s. The more rational and compassionate view is that we all have a responsibility to assist families in meeting theirs. When no families exist to do so, or those that do exist are unable or unwilling to do so, then it is our shared responsibility to step in and assist those innocent souls who some would leave to a life of suffering (and often of inflicting suffering on others, sometimes in ways which perpetuate the cycle of violence and despair across generations). The question should not be whether that is our shared responsibility, but rather how best to meet it.
It doesn’t matter that the sisters in this story were Australian nationals visiting the U.S. No one can deny that we have many like them that are home grown, and that our policies are implicated. On the news last night, there was a story of a woman who has had problems with alcohol abuse, and child abuse of her nine year old daughter, who apparently adored her daughter nonetheless, who was found, along with her daughter, in her running car in the garage of her home, both dead apparently from carbon monoxide poisoning (http://www.denverpost.com/news/ci_16653435). Friends and neighbors said that she loved her daughter too much to “take her with her” if she had wanted to commit suicide, but desperation isn’t that rational, and it’s not hard to imagine that, once the despair made suicide the only option the mother felt she had (if that was indeed the case), that same desperation could easily have made the thought of leaving her adored daughter behind to suffer the consequences as unbearable as life itself had become for her.
In an all-too-common story of deadly domestic violence, an ex-boyfriend, a military veteran, killed the girlfriend who ended their relationship (http://www.denverpost.com/news/ci_16643775). No member of the perpetrator’s family ever showed up for the three-week-long trial, and the mother of the victim said, with compassion, “I expect they were never there for you.” But we should have been. We can reduce the rate at which lives are destroyed by the combination of extreme individualism, a refusal to invest in proactive services (such as mental health service), insanely easy access to weapons and a culture that constantly glorifies violence. The fact that our rates of violent crime are much higher than those of other developed countries suggests that it’s not just the inevitable consequence of individual defects, but the very avoidable consequence of political choices and their cultural consequences.
A man, apparently also with mental health problems, who refused to leave his foreclosed home in Jefferson County not far from where I live required a SWAT team to evict him (http://www.denverpost.com/news/ci_16632232). The combination of economic stresses in this period of economic downturn, and a decrease rather than increase in our commitment to take care of one another, bode ill for the rate at which such events are likely to occur, and the rate at which they are likely to end badly.
There is no shame in evolving as a society to do more to mitigate such desperation, to be there for one another, and to create social institutions which identify, intervene, and offer assistance proactively at the earliest possible stage of the development of such problems. But the newly minted Republican Congressional majority in the House voted not to extend extensions of unemployment assistance (http://www.denverpost.com/nationworld/ci_16653692), when about 14.8 million Americans are unemployed (http://www.bls.gov/news.release/empsit.nr0.htm).
This commitment to leaving people to fend for themselves is justified by a highly questionable analysis of how to strike the optimal balance between debt and spending, and when to impose austerity v. when not to (http://coloradoconfluence.com/?p=1259). In the long run, investing in proactive human services, that reduce the private and public costs of unaddressed problems and the public costs of expensive reactive policies (e.g., the highest both percentage of population and absolute number of people incarcerated of any nation on Earth) not only increases human welfare, but it also improves our bottom line in the long run.
Those who hide behind the subterfuge that, sure, it’s our shared responsibility, but a responsibility best met through private charity and the decentralized volition of people of goodwill, are engaging in the convenient historical amnesia of how inadequately these needs were met prior to the utilization of government as an agent for meeting them, and how hollow such calls are when there is no private substitute anywhere in sight, capable of meeting these needs at anywhere near the level that government today currently inadequately meets them.
I am all for well-designed government-private sector partnerships, including with churches and other religious institutions, to address these problems. I have no inherent preference for government; just an inherent preference for facing our collective responsibilities to one another rather than finding excuses to shirk them. In fact, I’m a staunch advocate of strengthening our communities, and building greater non-governmental solidarity and mutual support into them, replacing something that has been lost in our forward march into extreme individualism. There are many pieces to the puzzle of addressing our failings as a society; improving the role of government, and integrating that role into the more organic social institutional materials with which government can and should work, is just one set of such pieces.
It’s time to stop the spiral down into cruel insanity, both the cases of individual insanity that we augment with our widespread ideological commitment to hyper-individualistic public policies of mutual indifference and disdain, and the collective insanity that those policies and that attitude are a symptom of.
Click here to buy my e-book A Conspiracy of Wizards for just $2.99!!!
